|
The transparent, gel-like vitreous was once considered innocuous, probably due to being nearly invisible and difficult to examine. However, advances in imaging capabilities have revealed that, in fact, the vitreous is an important ocular structure that plays an integral role in a variety of retinal diseases.1,2 As humans age, the gel-like vitreous slowly liquefies, the vitreoretinal interface weakens and the vitreous detaches.3,4 As this process takes place over time, many people will have stages of incomplete dehiscence, producing VMA. If this adhesion does not resolve itself or causes traction that results in visual distortions, it becomes symptomatic VMA. If the disruption to visual acuity is severe enough, it requires treatment.
Ocriplasmin Phase III Data
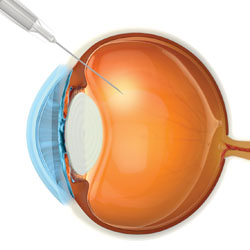
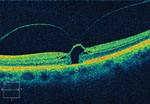
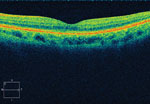
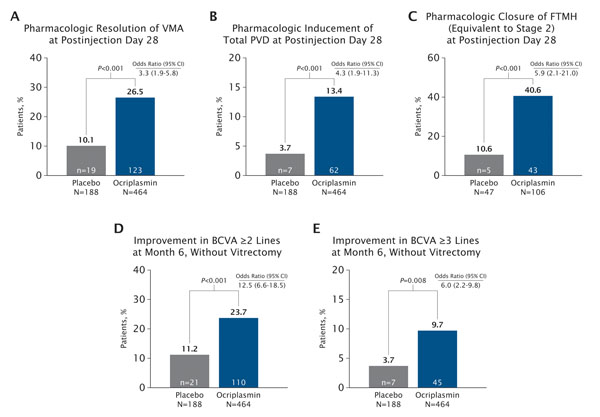
The Enzymatic Vitreolysis with Ocriplasmin for Vitreomacular Traction and Macular Holes study comprised two separate multicenter, randomized, double-blind clinical trials that treated 464 eyes with VMA with a single, 125 μg intravitreal injection of ocriplasmin (See Figure 1) and compared the results to 188 eyes that received a placebo injection. Vitreomacular adhesion resolved in 26.5 percent of ocriplasmin-injected eyes and in 10.1 percent of placebo-injected eyes (p<0.001, See Figure 2). Nonsurgical closure of macular holes was achieved in 40.6 percent of eyes in the ocriplasmin group, compared with 10.6 percent of placebo-injected eyes (p<0.001, See Figure 3).
Overall, the safety profile of ocriplasmin was very good. Ocular adverse events occurred in 68.4 percent of eyes in the ocriplasmin group and 53.3 percent of the placebo group. Most of the adverse events were mild in severity and transient, and the difference between groups was driven by temporary adverse events known to be associated with vitreous detachment. In fact, the incidence of serious ocular adverse events was 7.7 percent in the ocriplasmin group, as compared with 10.7 percent in the placebo group.
There were some instances of acute vision loss associated with an injection, but in all cases vision returned to baseline or an improvement over time. One hypothesis is that acute induction of posterior vitreous detachment caused these changes and that stabilization over time allowed for visual recovery.
| ||||
Which Patients Can Benefit
There are two primary indications for ocriplasmin. The first is for patients who have mild to moderate symptomatic VMA, and also have good visual acuity. Patients may be experiencing metamorphopsia, but test 20/40 or better on a Snellen visual acuity chart. Metamorphopsia can be tremendously disabling to functional capabilities, especially for those whose work requires them to read frequently or perform detailed visual tasks. However, vitrectomy surgery would not be a viable option for this group, because their vision is too good to risk the complications associated with surgery, including cataract formation, retinal tear, retinal detachment, bleeding and end-ophthalmitis.6 Historically, disease management for these patients has been careful observation, hoping the VMA would spontaneously resolve. However, the literature shows that many do progress and lose vision.7 The FDA approval of ocriplasmin provided surgeons with a minimally invasive means of treating these patients who previously had no viable option.
|
An example of the significance of this is with macular hole. Two main factors in the success of surgery for macular hole are baseline vision and size; thus delaying surgery could have a negative impact on the final prognosis. Patients and physicians will know quickly if the injection has worked, allowing them to proceed to surgery with minimal to no delay if necessary. In addition, a lack of response to the injection has no influence on the success rate of surgery.
During the preparation for similar clinical trials, I began to evaluate how many patients would fall into these two groups. I was surprised to realize that a small but steady number of candidates came into my clinic each week who might benefit from this treatment modality. These were patients who were either symptomatic from the VMA or vitreomacular traction, or suboptimally responsive to treatments for underlying disease (such as anti-VEGF treatment for neovascular AMD or diabetic macular edema). We do not know if the patients with underlying disease and VMA will respond better following this treatment, but it is a reasonable approach to relieve the VMA in an attempt to improve treatment response. Surgery is only a last-ditch option, as the durability of intravitreal injections decreases following vitrectomy.8-11 We do know that it is less effective in patients with epiretinal membranes. When patients were stratified, 37.4 percent of ocriplasmin-injected eyes and 14.3 percent of placebo-injected eyes achieved resolution of VMA when no ERM was present. This is in stark contrast to the 8.7 percent and 1.5 percent of eyes with ERM, respectively, that achieved resolution of VMA.
Future Indications
The potential for enzymatic vitreolysis presents an enormous shift in the current treatment paradigm, and I believe that our early use will be in the groups described above. We are still learning to identify VMA and recognize how many disease states it impacts. Going forward, we will formally investigate the anecdotal claims of the positive influence of resolution of VMA on response to anti-VEGF treatments. As we expand our use of ocriplasmin, we may modify the delivery method to achieve even greater efficacy at inducing resolution of VMA or full posterior detachment. REVIEW
Dr. Heier is the director of the Vitreoretinal Service at Ophthalmic Consultants of Boston; and the director of retinal research and co-director of the vitreoretinal fellowship at OCB/Tufts Medical School. He is a scientific consultant to Thrombogenics, Genentech and Regeneron. He also receives research income (through Ophthalmic Consultants of Boston) from Genentech and Regeneron. Contact him at jsheier@eyeboston.com.
1. Sebag J. Anomalous posterior vitreous detachment: A unifying concept in vitreoretinal disease. Graefe’s Arch Clin Exp Ophthalmol 2004;242:690-698.
2. Krebs I, Brannath W, Glittenberg C, et al. Posterior vitreomacular adhesion: A potential risk factor for exudative age-related macular degeneration? Am J Ophthalmol 2007;144:741-746.
3. Busacca A. La structure biomicroscopique de corps vitre normal. Ann. D’Oculist 1958;91:477-499.
4. Goldmann H. Senescenz des Glaskörpers. Ophthalmologica 1962;143:253-279.
5. Stalmans P, Benz MS, Gandorfer A, et al. Enzymatic Vitreolysis with Ocriplasmin for Vitreomacular Traction and Macular Holes. N Engl J Med 2012;367:606-615.
6. Park SS, Marcus DM, Duker JS et al. Posterior segment complications after vitrectomy for macular hole. Ophthalmology 1995;102:775-81.
7. Koerner F, Garweg J. Advances in the management of vitreomacular traction syndrome and macular hole. Dev Ophthalmol 1997;29:15-29.
8. Robison CD, Krebs I, Binder S, et al. Vitreomacular Adhesion in Active and End-Stage Age-related Macular Degeneration. Am J of Ophthalmol 2009;148:79-82.
9. Lee SJ, Lee CS, Koh HJ. Posterior Vitreomacular Adhesion and Risk of Exudative Age-related Macular Degeneration: Paired Eye Study. Am J of Ophthalmol 2009;147:621-626.
10. Mojana F, Cheng L, Bartsch DU, et al. The Role of Abnormal Vitreomacular Adhesion in Age-related Macular Degeneration: Spectral Optical Coherence Tomography and Surgical Results. Am J Ophthalmol 2008;146:218-227.
12. Lee SJ, Koh HJ. Effects of Vitreomacular Adhesion on Anti-Vascular Endothelial Growth Factor Treament of Exudative Age-related Macular Degeneration. Ophthalmology 2011;118:101-110.



