 |
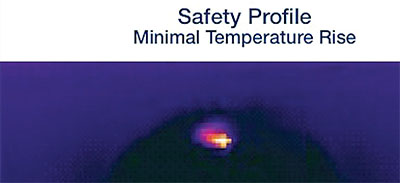
| IR image of capsulotomy being performed with CAPSULaser. The manufacturer says that a peak temperature of 67°C (white zone) is reached for an instant during the procedure. |
This state of affairs has been the status quo since the advent of femto in 2008, leaving room for the emergence of devices that promise to assist in the safe, fast creation of consistently strong and circular capsulotomies with less expense than that associated with femtosecond lasers.
Here are three products in development that aim to fill that void.
CAPSULaser
The CAPSULaser (CAPSULaser; Los Gatos, Calif.), the only laser in the group, relies on continuous thermal energy to create capsulotomies. After dilating the pupil and making sideport incisions, the surgeon stains the anterior capsule with trypan blue to visualize the CAPSULaser’s anatomical target. The CAPSULaser, which can be adjusted to select diameters from 4.5 to 7 mm, projects a pattern for the surgeon to follow with the laser. Unlike femto, this laser is continuous rather than pulsed. In one three-second pass, it creates a circular capsulotomy.
Richard Packard, MD, FRCS, FRCOphth, Prince Charles Eye Unit, King Edward VII Hospital, Windsor, England, notes that besides being fast and elegant, a CAPSULaser capsulotomy may be stronger and more elastic than those made by CCC or by femtosecond laser because its energy denatures the collagen. “In the region of irradiation, the laser energy facilitates the molecular phase change of the capsular collagen IV to elastic amorphous collagen. As the collagen undergoes this phase change it creates the capsulotomy with a rim that has a high degree of elasticity and tear strength associated with the amorphous collagen,” he explains. Dr. Packard adds that this strengthens the capsulotomy, potentially stabilizing the anterior capsule, which in turn can provide more consistent effective lens positioning.
CAPSULaser has completed preclinical testing on porcine and human cadaver eyes; Dr. Packard’s investigation of the device’s ability to make free-floating, centered and circular capsulotomies has been encouraging. Since the CAPSULaser uses low levels of continuous energy to make capsulotomies, the device momentarily raises the temperature of the the iris, corneal endothelium and retina by less than 0.2°C as measured by infrared imaging and thermocouple.
The CAPSULaser attaches to a standard surgical microscope, so its maker says it’s easily transportable and its use doesn’t require moving the patient to another location for the capsulotomy.
Zepto
The Zepto (Mynosys Cellular Devices; Fremont, Calif.) uses a method called “precision pulse capsulotomy.” The non-laser device consists of a console with a disposable handpiece equipped with a flexible nitinol ring designed to cut a capsulotomy cap about 5.2 mm in diameter. The ring folds to enter incisions as small as 2.2 to 2.4 mm, then springs back into shape. A suction cup placed over the capsular membrane pulls it gently towards the ring, which cuts a cap in four milliseconds with minimal disruption to the zonules. The user then discards the disposable cutting element on the tip of the handpiece, along with the removed capsular membrane slice.
Mark Kontos, MD, a senior partner at Empire Eye Physicians, which has offices in eastern Washington and northern Idaho, has a femto system but appreciates the simplicity and flexibility of the Zepto. During his time on Mynosys’s medical advisory board, Dr. Kontos had the opportunity to use the device in a laboratory setting. “Using the Zepto takes all of a couple of seconds,” he says. “You insert the device, center it on the lens, press the foot pedal and it all happens in seconds. It’s very quick and very easy, and it really doesn’t require any kind of new skill set from a cataract surgeon’s point of view: You’re just inserting another device inside the eye and the learning curve is extremely
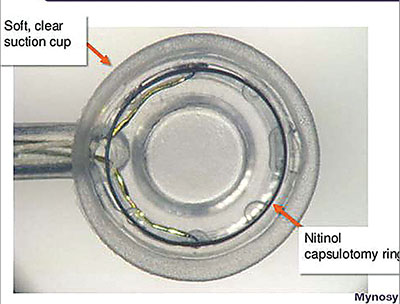 |
| The Zepto’s disposable cutting element includes a suction cup that gently draws the membrane towards the nitinol wire ring. |
Dr. Kontos also notes that surgeons can adapt their use of the Zepto as the case demands. “You can center it however you decide to—or decenter it as you want to. Let’s say that you have a patient who has a high angle kappa or something like that; if for some reason, you decide you want to center the capsulorhexis slightly nasal, you can. It gives you the flexibility of putting it more or less wherever you want,” he says.
The Zepto console is small, and the device doesn’t need to be attached to a microscope head, so it can potentially blend in with a practice’s established flow.
Mynosys says that the Zepto can produce consistently circular capsulotomies not attainable with manual CCC, and it doesn’t require a clear cornea. “You could put it into an eye with a cornea that has very poor visibility and still be able to get a perfect capsule out of it,” says Dr. Kontos. He adds that the Zepto can make a successful capsulotomy in poorly dilated pupils more easily than a laser can. “The pupil will come down, and sometimes it will come down to the point where it’s very difficult to do a laser treatment. With the Zepto, you can slide it underneath the iris, so you can still make a perfectly round, centered capsulotomy even if you don’t have a widely dilated pupil. It doesn’t damage the iris in any way.”
The Zepto produces maximum temperature increases in the eye of no more than 2.01°C, according to Mynosys. The precision pulse capsulotomy method employed by the Zepto created smooth, flexible capsulotomy edges with tear strength exceeding that of edges made by manual CCC and femtosecond laser in one U.S. study of cadaver eyes partially sponsored by Mynosys.1
Mynosys is currently seeking a 510(k) clearance from the FDA, and the Zepto is currently in use abroad.
ApertureCTC
This device’s maker, International BioMedical Devices (Charleston, S.C.), says the “CTC” stands for “continuous thermal capsulotomy,” which
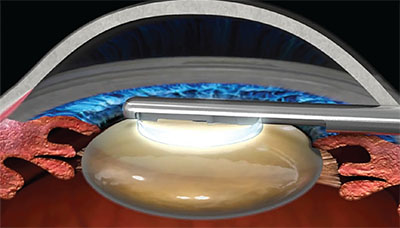 |
| An illustration of the ApertureCTC’s thermal element in contact with the caspsule. The disposable ring provides continuous, all-points contact with the membrane to cut a uniformly smooth and circular capsulotomy. The rings are available in a range of diameters. |
The ApertureCTC handpiece is used with disposable steel rings ranging from 4.5 to 6.5 mm in diameter. In use, the ring attaches to the tip of the 1.2-mm handpiece and retracts at the sides to fit through a small incision. Once over the anterior capsule, the user expands the ring back out to its original shape. The ring delivers thermal energy to the capsular membrane and captures the circular cap for removal. Because it relies on thermal energy, and all points of the ring are in contact with the membrane at all times during the capsulotomy, Mark Packer, MD, FACS, says the procedure can be completed in milliseconds under the protection of an OVD. “As the ring is retrieved, it automatically captures and removes the perfectly circular cap,” notes Dr. Packer, who is chief medical officer for IBMD. “The disposable tip is discarded after the case, and the reusable handpiece is sterilized in standard fashion.
“The key features of the ApertureCTC are its continuous 360° thermal element, which overcomes the inevitable gap required by radiofrequency devices with loop-wire or ring cutting elements; and its uniform contact with the anterior capsule, which obviates the necessity for vacuum suction,” he continues. “This technology has the potential to ensure safer cataract surgeries and may also provide more predictable visual outcomes for patients.
“We are currently in preclinical- stage testing,” says Dr. Packer of the device’s ongoing development.
Dr. Packard is a consultant and equity shareholder in CAPSULaser. Dr. Kontos reports no relevant financial interests. Dr. Packer is the chief medical officer of International BioMedical Devices, Inc.
1. Thompson VM, Berdahl JP, Solano JM, Chang DF. Comparison of manual, femtosecond laser, and precision pulse capsulotomy edge tear strength in paired human cadaver eyes. Ophthalmology 2016 Feb;123:2:265-74.


