 |
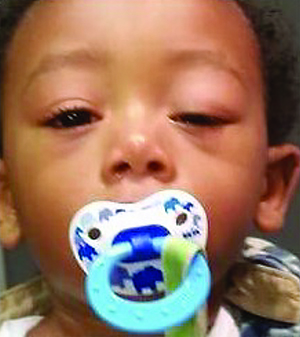
| Figure 1. Child with left congenital ptosis with absent left upper lid crease, using compensatory chin-up position. (Image courtesy Anne Barmettler, MD.) |
The majority of congenital ptosis is unilateral, and it can occur as an isolated phenomenon or in association with other ocular or systemic findings.1,3-8 Although the etiology is classically thought to be myogenic in nature, more recent reports have suggested that disordered innervation during embryonic development may be the underlying cause.6 Additionally, Mohammed Alshehri, MD, and colleagues examined Müller muscle in a series of 12 patients with congenital ptosis and found structural abnormalities compared to six control patients with aponeurotic ptosis.9 Several genes have been implicated in isolated congenital ptosis, including autosomal dominant inheritance and X-linked dominant inheritance.3,6 Congenital ptosis can be associated with Blepharophimosis, ptosis, and epicanthus inversus (BPEI) syndrome; Duane Retraction syndrome; congenital fibrosis of the extraocular muscles; Marcus-Gunn jaw-winking syndrome; Congenital Horner’s syndrome; and strabismus, among others.1,3-8
Evaluation
Take a thorough history on every child who presents with ptosis. Inquire about the age of onset and any fluctuations or progression, pupil asymmetry, motility or alignment abnormalities, trauma or allergic reactions. Additional history should focus on medical history, including birth and development, family history and review of systems. Photographs of the child at a younger age or of family members may be helpful.
On examination, first observe the child, looking for anomalous head position, including compensatory chin-up position, and spontaneous frontalis use (See Figure 1). Obtain visual acuity and cycloplegic refraction, and assess pupils, looking for anisocoria, motility and alignment. With the head in neutral position, the frontalis immobilized to maintain the brow in normal anatomic position, and the patient fixating at distance, hold a ruler vertically next to the eye. Measure the distance between the upper lid margin and the corneal light reflex to the nearest 0.5 mm for margin reflex distance (MRD)1, and the distance between the lower lid margin and the corneal light reflex for MRD2. Ptosis is considered mild at ≤2 mm, moderate at 3 mm and severe at ≥4 mm, as classified by Crowell Beard, MD.15
In the same position, with the frontalis fixated, measure levator function in mm as the excursion of the upper lid margin from maximal downgaze to maximal upgaze. Levator function is subdivided into excellent (≥13 mm), good (8 to 11 mm), fair (5 to 7 mm), and poor (≤4 mm).7,10 Look for lid lag—poor movement of the lid with the globe—in downgaze. In unilateral cases, the ptotic side will often be higher in downgaze due to poor motility of the fibrotic levator muscle. Assess frontalis function and the amount of lagophthalmos.
Consider Hertel exophthalmometry if pseudoptosis secondary to contralateral proptosis is a concern, although this can be difficult in young children. Proptosis can be assessed grossly from a worm’s eye view. Palpate the eyelids and orbital rims for masses, and examine the lids for erythema or edema and lid crease. The lid crease is often poorly formed or absent with congenital ptosis, in contrast to the higher lid crease typically seen with involutional aponeurotic ptosis.
Determine whether the patient has an intact Bell’s phenomenon, as a poor Bell’s phenomenon increases the risk of exposure keratopathy after surgical intervention. A complete anterior segment exam, especially of the tear lake, corneal surface integrity and iris coloration, and dilated fundus exam should be completed as well.7
Differential Diagnosis
The differential diagnosis includes traumatic ptosis; mechanical ptosis; neurogenic ptosis; aponeurotic ptosis; myasthenia gravis; blepharochalasis; chronic progressive external ophthalmoplegia; preseptal or orbital cellulitis; allergic dermatitis; orbital mass; conjunctivitis; corneal foreign body or ulcer; and pseudoptosis.
Management
 |
| Figure 2. Patient with bilateral congenital ptosis, marked for frontalis sling in pentagonal pattern. (Image courtesy American Academy of Ophthalmology ONE images.) |
Surgical Options
The surgical method depends on both the severity of ptosis and the amount of levator function. Several common options will be discussed; the Fasanella-Servat procedure and the Müller muscle-conjunctival resection will not be covered here as they are most useful in mild ptosis with good levator function, which is not characteristic of most cases of congenital ptosis. Congenital ptosis as part of syndromes such as BPEI and Marcus-Gunn jaw-winking syndrome require more complicated surgical planning and are outside the scope of this article.
Frontalis Sling
Frontalis sling is one of the most commonly used operations for poor levator function. The upper lid is linked to the frontalis, such that contracting the frontalis will simultaneously elevate the lid. There are multiple variations in technique. The sling can be placed in pentagon (See Figure 2), single-triangle, or double-triangle configuration via supraciliary stab incision or lid crease incision.3,7 The material can be sutured to the tarsal plate, which was recently found by Dr. Ibrahim Bulent Buttanri and colleagues to produce a higher success rate than unsutured silicone rods, with a non-statistically significant higher success rate using braided polyester versus monofilament polypropylene.13
The material for suspension can also vary, including autogenous or banked fascia lata; silicone rods; polyester; collagen; silk; stainless steel; monofilament nylon; polytetrafluoroethylene; and polypropylene.3 Some surgeons consider autogenous fascia lata the best material, due to its biocompatibility and longevity, although it requires a second surgical site and patients must be at least 3 years old to provide a graft of adequate length.3 Banked fascia lata, although felt to be a good alternative to autogenous fascia lata, has a long-term success reported only around 50 percent, possibly due to early resorption.14 Silicone rods are one of the most frequently used alloplastic material as their elastic nature allows both for good eyelid height (See Figure 3) and complete eyelid closure, although as with all alloplastic materials, there is a risk of infection, inflammation, granuloma formation and extrusion.3,14
Overall, the frontalis sling is considered effective and well-tolerated, and has the advantage of being adjustable postoperatively, depending on the material used. In addition to those mentioned above, potential risks include lagophthalmos, lid crease distortion and poor lid-globe apposition.
Levator Resection, Advancement
Levator resection and advancement can be considered in patients with levator function ≥5 mm.3,7 Levator resection can be approached either anteriorly or posteriorly, although the anterior approach provides better exposure and the ability to reform the lid crease, and allows for greater degrees of levator resection.7 After the levator is exposed, it is either plicated or resected, then sutured to the tarsal plate with partial-thickness bites, typically with nonabsorbable sutures.3,7 The sutures can be initially tied in temporary fashion and adjusted to the desired contour and height. There are various methods to calculate the amount of levator to resect. Intraoperatively, you can set the upper lid margin at the superior corneal limbus for severe ptosis and mid-pupil for mild ptosis with good levator function.7 Alternatively, quantitative algorithms have been published based on the severity of ptosis and degree of levator function, including a simple recommendation to resect 4 mm of levator for every 1 mm of ptosis.3 Of note, some surgeons will still use a levator resection, with or without a tarsectomy, for patients with severe ptosis and poor levator function, with reported good success.3
Whitnall Sling
 |
| Figure 3. A child with left congenital ptosis status post left frontalis sling, with improved left eyelid position and presence of lid crease. (Image courtesy Anne Barmettler, MD.) |
Modified Tarsal Resection
An alternative for patients with fair levator function is a modified tarsal resection with graded levator advancement, as described by Sarit Patel, MD, and colleagues. From an anterior approach, the levator aponeurosis is exposed and disinserted from the tarsus, then separated from Müller muscle. The anterior face of the tarsus is exposed. A predetermined amount of tarsus and Müller (in a 1:2 ratio) to be excised is marked, depending on the amount of ptosis, then tarsus, Müller muscle and conjunctiva is resected en bloc. The inferior edge of Müller muscle and conjunctiva is then advanced to the new superior tarsal border with absorbable sutures. Levator aponeurosis is then advanced to the anterior face of the tarsus and adjusted to set the upper lid margin at the superior corneal limbus. All patients had mild lagophthalmos in the immediate postoperative period only, with good results in 25 of 30 patients (30 of 36 lids).10
Congenital ptosis can occur in isolation or in conjunction with other ophthalmic or systemic findings. It can be both amblyogenic and a cause of psychosocial distress. Although some cases can be monitored and managed with amblyopia treatment until the child is older, surgery should be done sooner for worsening amblyopia or compensatory positioning that is excessive or interferes with function. Because the levator muscle is often anomalous and poorly functioning, surgical management can be challenging and should be approached on a case basis. REVIEW
Dr. Liao is an oculoplastics attending surgeon at the New York Eye and Ear Infirmary of Mt. Sinai.
1. Griepentrog GJ, Diehl NN, Mohney BG. Incidence and demographics of childhood ptosis. Ophthalmology 2011;118:1180-1183.
2. Hu D. Prevalence and mode of inheritance of major genetic eye diseases in China. J Med Genet 1987;24:584-588.
3. SooHoo JR, Davis BW, Allard FD, Durairaj VD. Congenital ptosis. Surv Ophthalmol 2014;59:483-492.
4. Griepentrog GJ, Mohney BG. Strabismus in childhood eyelid ptosis. Am J Ophthalmol 2014;158:208-210.
5. Berry-Brincat A, Willshaw H. Paediatric blepharoptosis: A 10-year review. Eye 2009;23:1554-1559.
6. McMullan TFW, Robinson DO, Tyers AG. Towards an understanding of congenital ptosis. Orbit 2006;25:179-184.
7. Ahmadi AJ, Sires B. Ptosis in infants and children. Int Ophthalmol Clin 2002;42:15-29.
8. El Essawy R, Elsada MA. Clinical and demographic characteristics of ptosis in children: A national tertiary hospital study. Eur J Ophthalmol 2013;23:356-360.
9. Alshehri MD, Al-Fakey YH, Alkhalidi HM, et al. Microscopic and ultrastructural changes of Muller’s muscle in patients with simple congenital ptosis. Ophthal Plast Reconstr Surg 2014;30:337-341.
10. Patel SM, Linberg JV, Sivak-Callcott JA, Gunel E. Modified tarsal resection operation for congenital ptosis with fair levator function. Ophthal Plast Reconstr Surg 2008;24:1-6.
11. Griepentrog GJ, Diehl N, Mohney BG. Amblyopia in childhood eyelid ptosis. Am J Ophthalmol 2013;155:1125-1128.
12. Stein A, Kelly JP, Weiss AH. Congenital eyelid ptosis: Onset and prevalence of ambyopia, associations with systemic disorders, and treatment outcomes. J Pediatr 2014;165:820-824.
13. Buttanri IB, Serin D, Karslioglu S, et al. Effect of suturing the silicone rod to the tarsal plate and the suture material used on success of frontlias suspension surgery. Ophthal Plast Reconstr Surg 2014;29:98-100.
14. Bansal RK, Sharma S.. Results and complications of silicone frontalis sling surgery for ptosis. J Pediatr Ophthalmol Strabismus 2015;52:93-97.
15. Beard, C. A New Classification of Blepharoptosis. Int Ophthalmol Clin 1989;29:214-216.


