A 75-year-old Caucasian female presented to the Retina Service at Wills Eye Institute for a second opinion with a red “swollen” right eye associated with blurred vision for the past three months. She had previously been under the care of an outside ophthalmologist who diagnosed her with scleritis of the right eye and anterior uveitis of both eyes.
Her clinical course was notable for resolution of the anterior uveitis after the initiation of difluprednate, but with persistent injection of the right eye despite dosing at four times each day. She also required therapy with aqueous suppressants in both eyes for elevated intraocular pressure. A laboratory workup for scleritis included FTA, ANCA and chest radiograph; all were negative. She endorsed a recent history of shortness of breath, while denying ocular pain, photophobia, diplopia, tinnitus, headache, weakness, paresthesias, arthralgia, diarrhea or bloody stool, facial pain or nasal discharge. She denied any recent trauma.
Medical History
The patient noted a history of strabismus and amblyopia in the left eye, with multiple muscle surgeries as a child. Past medical history was notable for hypertension, hyperlipidemia and hospitalization two weeks prior for deep venous thrombosis with pulmonary embolism severe enough to cause right heart strain. Ocular medications included difluprednate four times a day in the right eye, timolol-dorzolamide twice a day in the right eye, and timolol twice a day in the left eye. Systemic medications included amlodipine, simvastatin and warfarin. She denied any smoking history.
Examination
Ocular examination revealed best corrected visual acuity of 20/80 in the right eye and 20/400 in the left eye. There was no afferent pupillary defect. A comitant left exotropia was noted, with full ocular motility of both eyes. Visual fields were full in both eyes by confrontational testing. Applanation tonometry measured an intraocular pressure of 23 mmHg in the right eye and 17 mmHg in the left eye. Proptosis of the right eye was noted and confirmed by Hertel exophthalmometry that measured 20 mm on the right versus 13 mm on the left with a base of 113 mm. An orbital bruit was not appreciated.
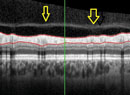
Slit-lamp examination revealed normal adnexa and eyelids. The right eye exhibited diffusely dilated and tortuous episcleral vessels that were noted to have a “corkscrew” appearance. There was no tenderness on palpation of the right globe over a closed eyelid. The conjunctiva, episclera and sclera of the left eye were white and quiet. The anterior chamber of both eyes had trace cell without flare. Posterior chamber intraocular lenses were present in both eyes. Posterior exam of the right eye revealed a mildly edematous optic disc with shunt vessels, dilated and tortuous retinal veins in all four quadrants, flame shaped and dot hemorrhages, and macular edema. The left eye showed a tilted nerve with an otherwise normal-appearing fundus. Optical coherence tomography was performed, showing macular edema in the right eye. Fluorescein angiography of the right eye revealed a delayed arteriovenous phase, late macular and disc leakage and some areas of nonperfusion.
What is your differential diagnosis? What further workup would you pursue?