Vascular endothelial growth factors are 40kDa dimeric glycoproteins1 implicated in the pathophysiology of multiple leading causes of blindness, including neovascular, or wet, age-related macular degeneration and diabetic retinopathy,2 among others. These molecules play a vital role in angiogenesis3 and have been detected in ocular fluid samples in proliferative diabetic retinopathy, iris neovascularization and ischemic central vein occlusion.4 Thus, they have been the target of multiple medications for the last two decades after the approval of the first anti-VEGF, pegaptanib, in ophthalmic use in the early 2000s.5,6 Since then, other anti-VEGF medications have been developed and have been used in a multitude of retinal diseases. Here, we’ll explore one of the newest drugs being studied in the battle against these diseases: tyrosine kinase inhibitors.
The Anti-VEGF Landscape
The current limitations of anti-VEGF injections lie in the frequency at which they have to be administered. Even with treat-and-extend protocols, the number of patients maintained at prolonged intervals is variable,7 and the average number of injections with this protocol is around 13 for the first two years.7-9 The frequency of injections can place a psychological and financial burden on the patients and caregivers, affecting treatment compliance.10 Furthermore, there are possible complications associated with the injections, including endophthalmitis, intraocular inflammation, vasculitis, tractional/rhegmatogenous retinal detachment, increased intraocular pressure and ocular hemorrhage.11,12
This led to the attempt to reduce the treatment burden and to develop sustained delivery systems.13 For example, the port delivery system for ranibizumab (Susvimo) was FDA approved for the treatment of nAMD, as a surgically implanted refillable reservoir of anti-VEGF.14 However, it was associated with a higher risk of endophthalmitis and hemorrhage with earlier surgical techniques, and was temporarily recalled due to reported septum dislodgment15 prior to recirculation.
Moreover, like VEGF, platelet-derived growth factor (PDGF) is important in angiogenesis.16 It plays a role in pericyte recruitment and vascular maturation,17,18 and we know from animal models that the paucity of pericytes made vessels more prone to regression with VEGF inhibitors.19 In fact, a recent clinical trial (Phase IIb) on dual VEGF/PDGF inhibition in wet AMD showed favorable results relative to anti-VEGF monotherapy.20 However the Phase III clinical trial didn’t achieve its primary endpoint.
Other potential culprits are the angiopoietins (Ang) which have also been implicated in angiogenesis22 and increased inflammatory signaling.23 Dual inhibition of VEGF and Ang2 (Faricimab) has shown visual and anatomic benefits at more extended intervals in nAMD and DME in recent trials.24,25 Thus emerged the importance of inhibiting multiple targets in these pathologies.
What are Tyrosine Kinase Inhibitors?
The VEGF family includes VEGF A, B, C, D and E, as well as placental growth factor (P1GF), which bind to different forms of VEGF receptors (VEGFR) that have been identified. These include VEGFR 1, 2 and 3. The most important players in angiogenesis are VEGF-A and its receptors VEGFR-1 (fms-like tyrosine kinase-1 or Flt-1) and 2 (kinase insert domain-containing receptor or KDR), both receptor tyrosine kinases (RTK).2,26–28 This family of receptors has been implicated in angiogenesis, tumorigenesis and metastasis.29 P1GF can also play a role through synergism with VEGF in pathological conditions, thus increasing angiogenesis and plasma extravasation.30
The previously mentioned PDGF and angiopoietins bind to PDGF receptors (α and β, belonging to the class III receptor tyrosine kinases16) and the Tie (tyrosine kinase with immunoglobulin and epidermal growth factor homology domains31) receptor family, respectively. While Ang1 promotes vascular stability in physiological conditions through binding to Tie2, the increase of Ang2 in disease conditions, eg., hyperglycemia, leads to vascular destabilization and enhanced response to VEGF A, thus increasing vascular leakage and neovascularization.31,32 Inhibition of Ang2 in animal models leads to inhibition of neovascularization promoted by VEGF.33
Other factors involved in angiogenesis include fibroblast growth factor (FGF) which also binds to an RTK.34 Animal models with pancreatic cancer subjected to treatment with VEGF inhibitors showed the appearance of resistance to this treatment in late stages, with reactivation of angiogenesis.35 This was due to the presence of other factors which promoted angiogenesis, including FGF.35
Similar to the initial development of VEGF inhibitors in cancer treatment, tyrosine kinase inhibitors were studied in oncology to target angiogenesis. Instead of blocking the ligand, TKIs exhibit their effects through inhibition of downstream intracellular signaling that follows ligand-receptor binding.27 The first approved drug in this family was imatinib, which paved the way for targeted medicine, and improved survival rates and quality of life.36 This family of drugs can range in selectivity, and some can target multiple receptors.29 In fact, TKIs that targeted both VEGFR and PDGFR showed better results than inhibition of either separately.37
 |
TKIs in Retinal Diseases
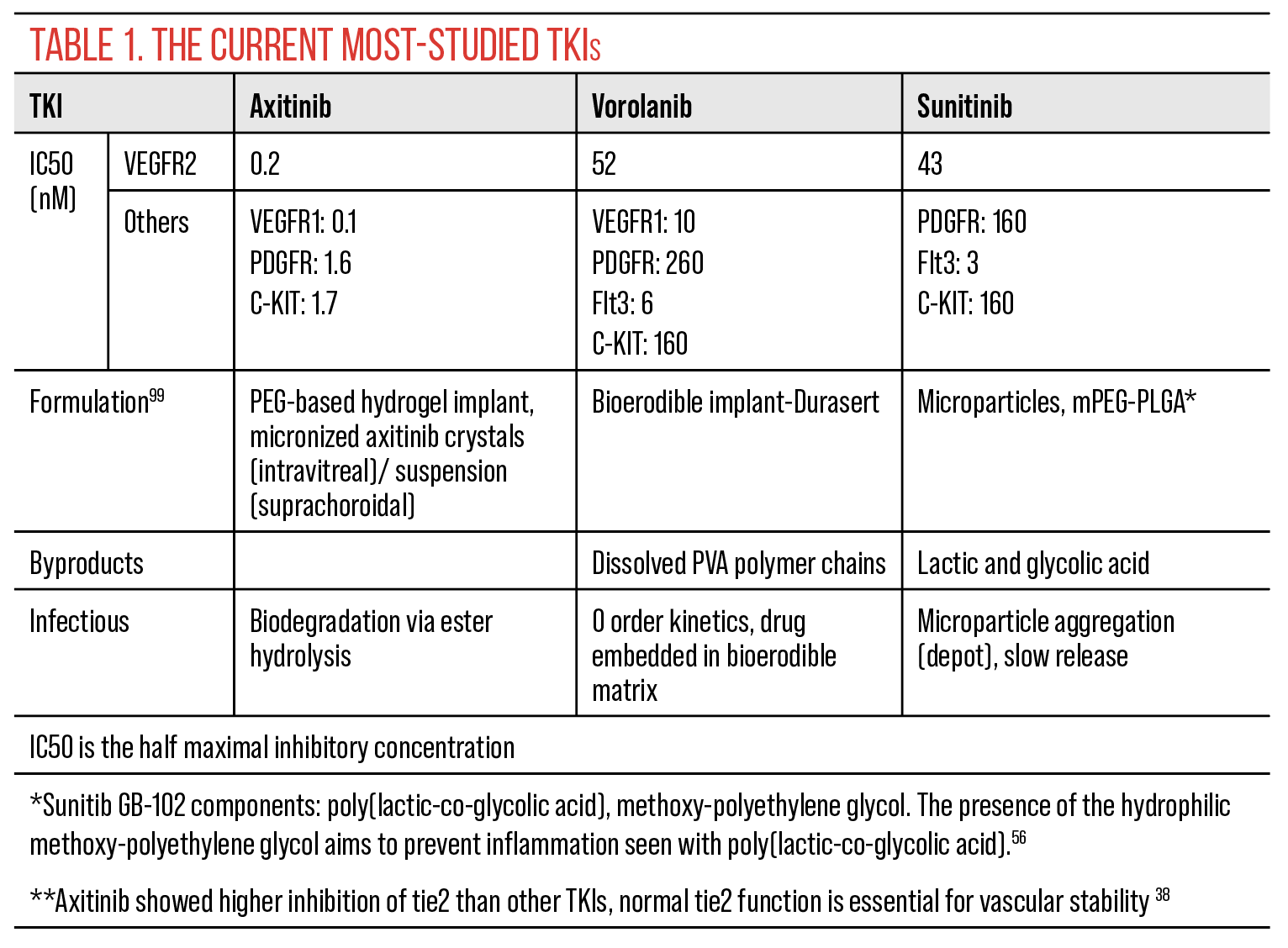
Several tyrosine kinase inhibitors have recently been studied in retinal diseases. These include axitinib, sunitinib, vorolanib, anlotinib and pazopanib. The three mainly studied drugs, and their formulations and affinities can be found in Table 1. While all show potent inhibition of VEGFR, axitinib had the strongest effect.38 The different formulations aim to ensure prolonged release, and therefore longer-lasting effect, of the active drug.
• Axitinib. Axitinib is a potent inhibitor of VEGFR 1, 2, and 3, with its oral formulation approved in the treatment of renal cell carcinoma, and used in the treatment of other malignancies as well.39 It also targets PDGFR, though is a less potent inhibitor of this receptor than initially found in in vitro studies.40
Clinical trials involving this drug can be seen in Table 2. In a Phase I U.S.-based clinical trial of axitinib in nAMD, a single bioresorbable hydrogel implant of the drug (OTX-TKI, Ocular Therapeutix), followed by an injection of aflibercept at one month, showed similar outcomes in visual acuity and central thickness in comparison with aflibercept every eight weeks.41,42 Axitinib was well-tolerated with no reported adverse events, and with a decrease in treatment burden, demonstrated by 80 percent rescue-free participants in the treatment arm at 24 weeks and 60 percent rescue-free at week 52. Safety data showed the implant was well-tolerated.
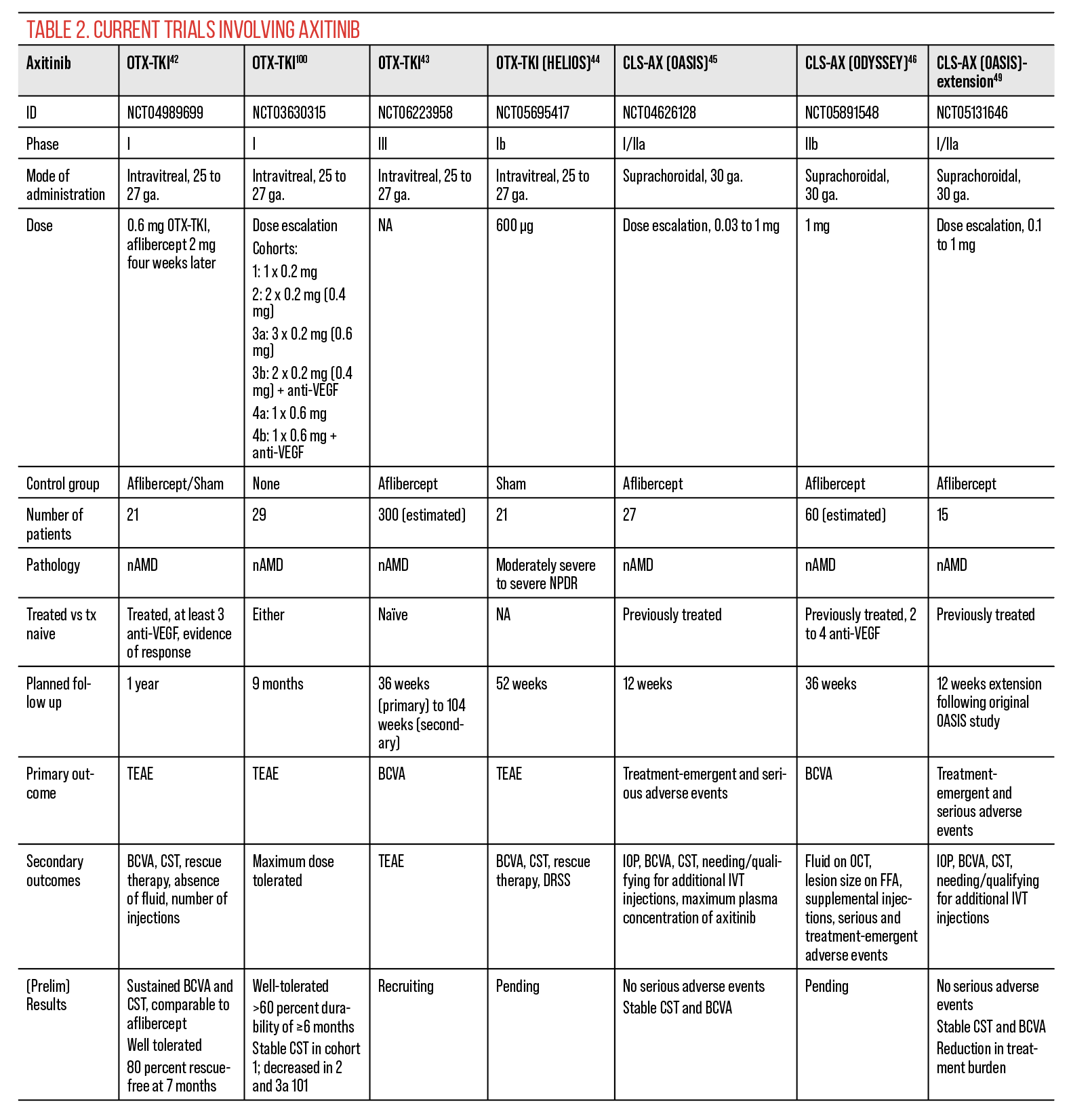 |
A Phase III trial (SOL-1 is currently recruiting subjects with treatment-naïve nAMD for axitinib injection with 151 subjects enrolled as of June 2024; results have yet to be reported.43 Other trials underway for this drug include moderately severe to severe non-proliferative diabetic retinopathy; a Phase I trial (HELIOS) demonstrated that 23.1 percent (n=3) of subjects receiving an axitinib implant had ≥2-step improvement in the diabetic retinopathy severity scale compared to zero in the sham group at week 48.44
Other modes of administration of axitinib currently in trial include suprachoroidal injection (CLS-AX, Clearside Biomedical).45,46 The advantages of this minimally invasive method are numerous, including decreased risk of infection, potential prolonged release of the drug, compartmentalizing the drug near the target tissue and decreased floaters.47 Phase I/IIa trials (OASIS) of CLS-AX have demonstrated that in anti-VEGF treatment-exposed sub-responders, 83 percent of patients went ≥4 months without additional treatment, 67 percent went ≥6 months without additional treatment, and 50 percent didn’t require additional treatment for >6 months. In the extension of this study, the different axitinib dose cohorts showed no adverse events and a decrease in treatment burden at six months.48,49 A Phase IIb randomized, double-masked multicenter clinical trial comparing CLS-AX 1 mg suprachoroidal injection to intravitreal 2 mg aflibercept injection for neovascular AMD in eyes previously treated with standard of care intravitreal anti-VEGF is currently underway. Outcome measures will report change in best-corrected visual acuity over 36 weeks, need for supplemental treatment, and treatment burden as quantified by total number of injections over study period.
• Sunitinib. Sunitinib targets VEGFRs, PDGFR, stem cell growth factor receptor (KIT) and FLT3.50 It’s used in oncology in the treatment of metastatic renal cell carcinoma, gastrointestinal stromal tumors, lung cancer and pancreatic neuroendocrine tumors.50–53 Preclinical trials investigated biodegradable microparticles of sunitinib, which aggregated in a depot in the inferior vitreous after intravitreal injection, and slowly released the active drug. The trials showed that this medication was nontoxic and retained active levels of the drug at the level of the retina and RPE/choroid for at least four months.54 In fact, due to its reversible binding to melanin, sunitinib was found to remain up to six to seven months in the RPE/choroid of pigmented rabbits.55
In animal models, sunitinib microparticles also reduced photoreceptor cell death,56 and in a separate study, sunitinib had protective effects on retinal ganglion cells in an animal model of nonarteritic optic neuropathy.57 Clinical trials involving sunitinib can be seen in Table 3, including trials in wet AMD, diabetes and retinal vein occlusion. A Phase I study showed tolerability of sunitinib (GB-102, Graybug vision), an injection formulated for twice-yearly dosing. However, there was evidence of migration of bioabsorbable particles into the anterior chamber in 28 percent of patients, which was self-limited.58 A Phase IIb study (ALTISSIMO) of the drug versus aflibercept showed that the median time to rescue was five months for the GB-102 1 mg group. The lower dose was well-tolerated with mild-to-moderate adverse events. It was also noted that there was a decrease in injection frequency by 58 percent compared to before enrollment. The CST was comparable in both groups, while the BCVA showed lower numbers in the GB-102 arm by approximately nine ETDRS letters. This was speculated to be influenced by a number of patients within the study arm that either had prior poor response to anti-VEGF, or had ocular adverse events during the study, whether related or not to the microparticles.59–61 With changes to the drug formulation in this phase, there were fewer cases of migration into the anterior chamber: <10 percent in the 1-mg arm.
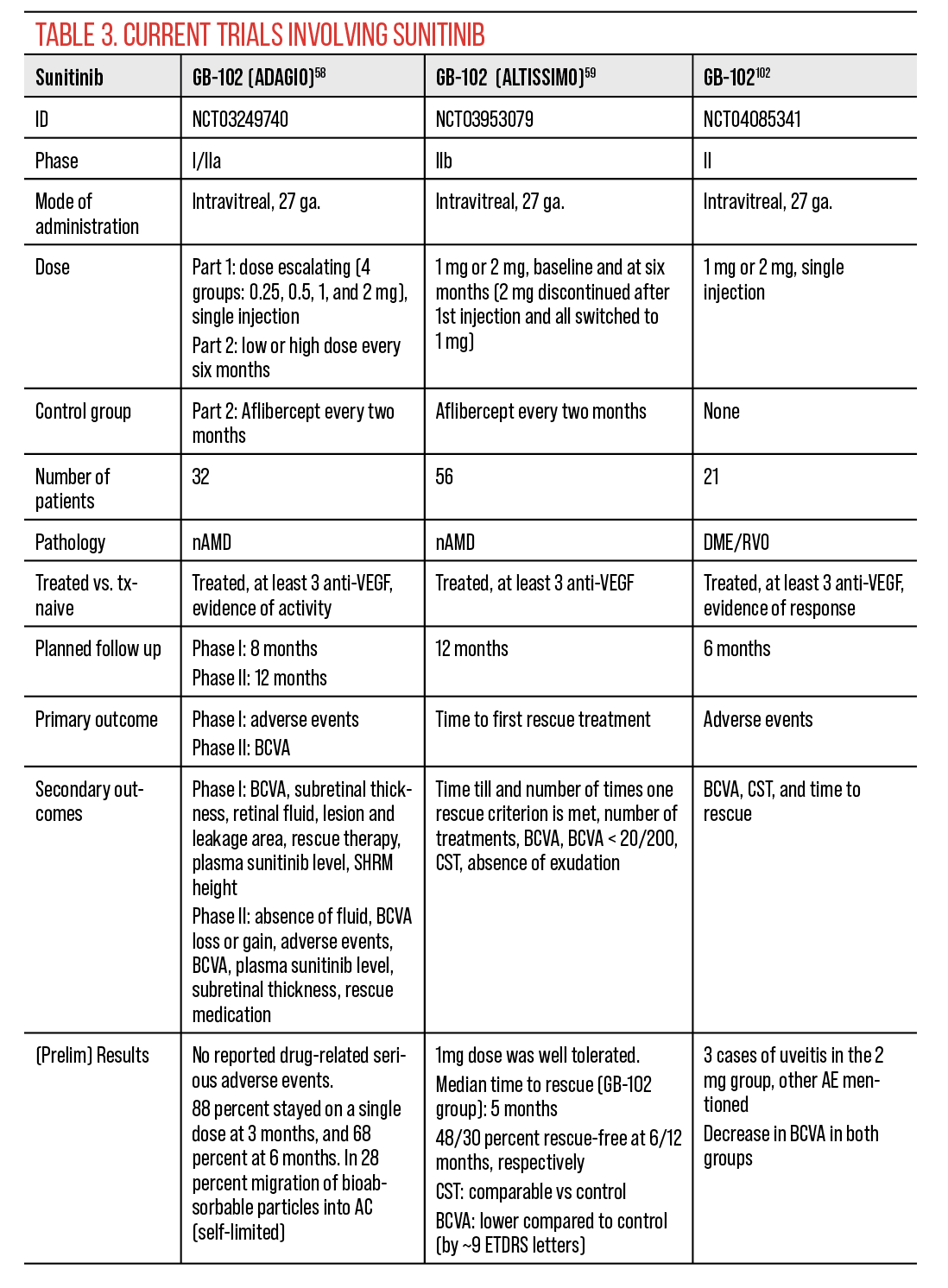 |
At the conclusion of this initial “core study” of GB-102, an “extension study” was performed, with a six-month follow-up without additional treatment.62 This included patients who didn’t require additional therapy at the 12-month follow-up, of which 11 patients were in the GB-102 1-mg arm. Fifty-five percent of this arm retained a treatment duration of 12 months or longer, with stable BCVA and CST.62 For those patients, the yearly injection burden was reduced by 73 percent. This led to the discontinuation of the work on GB-103, a second-generation formulation with a potential annual injection of the drug, which maintained active levels for five months in the retina and RPE/choroid, and thus supplementary five to six months relative to GB-102.63 However, more recently, Graybug, now acquired by CalciMedica, stopped the development of GB-102.
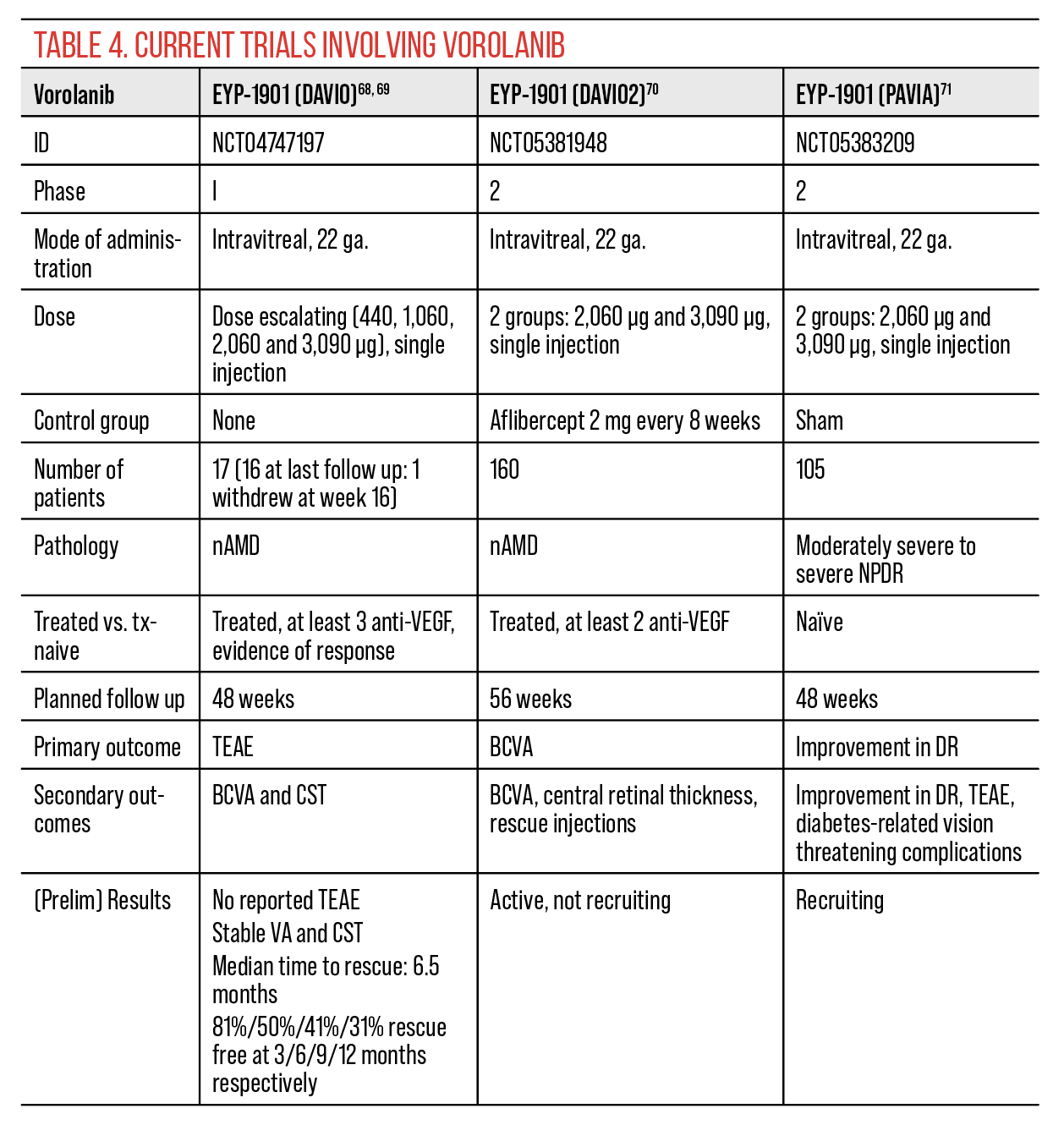
• Vorolanib. Vorolanib is a small molecule TKI, based on the sunitinib scaffold, aiming for lower tissue accumulation.64 It inhibits VEGFRs, PDGFR and cKIT, but not Tie2, and is used in multiple types of solid tumors.64,65 Clinical trials with vorolanib in retinal pathology included an oral formulation, which will be discussed later, and in-office intravitreal injections using the sustained release Durasert platform (EYP-1901, EyePoint Pharmaceuticals). This platform can be found in other drug formulations (e.g., Yutiq and Iluvien), where in contrast to EYP-1901 for vorolanib, it’s covered with a non-erodible polyimide shell.66 The Durasert E used for vorolanib is biodegradable.
A Phase I study (DAVIO) on the safety of vorolanib (EYP-1901; Duravyu) in wet AMD, reported no drug-related adverse events, with stable CST and more than a 70-percent reduction in treatment burden at six and 12 months.67–69 Phase II trials of this drug in wet AMD and moderately severe to severe NPDR are ongoing,70,71 and are expected to start recruiting in diabetic macular edema.72 Six-month results from a Phase II trial in nAMD (DAVIO2) showed noninferiority of Duravyu to aflibercept in the two dose groups and more than 80-percent decrease in treatment burden.73 There was a favorable safety profile. The Phase III program for EYP-1901 for wet macular degeneration is planned to commence in the second half of 2024. Phase II trials are currently underway for the use of Durasert for NPDR and DME.
 |
Other formulations of TKIs
Besides the aforementioned formulations of the TKI in the form of injections, sunitinib, pazopanib, and axitinib aqueously dispersed eyedrops were compared to aflibercept in an animal model of wet AMD.77 They showed comparable efficacy to aflibercept in reducing the size of the CNV, and statistically significant efficacy relative to regular sunitinib eye drops. In contrast, a Phase II trial of an ophthalmic oily suspension of regorafenib, a TKI that targets VEGFRs, PDGFR, tie2, KIT and FGFR,78 was terminated because of lack of efficacy, likely related to poor absorption of the drug into the back of the eye.79,80 Despite promising results on CNV in animal models,81 the prior eye-drop form of pazopanib, though well tolerated, showed a lack of efficacy at 12 months in wet AMD and the trial was terminated.82,83
Another trial comparing pazopanib drops with ranibizumab injections failed to demonstrate a benefit in reducing the injection burden with the former treatment.84 Oral pazopanib, a TKI targeting VEGFRs, PDGF, cKIT and FGF,85 was also studied in the treatment of AMD, and a Phase I trial showed tolerability of the drug and promising results.86–88 However, it was limited by the length of the follow-up and the number of participants.
Oral vorolanib (X-82, CM082) has also been studied in wet AMD and myopic CNV,89–93 and while there have been reductions in CST and CNV area, the trials have recorded systemic treatment-related adverse events.94,95
Moreover, oral sunitinib, while potentially helpful in certain cases of peripapillary retinal capillary hemangioblastomas in von Hippel Lindau, resulted in multiple side effects that might limit its use in this formulation for retinal disease.96
It’s also worth noting, however, that while rare, oral TKIs have been associated with ocular complications, including serous retinal detachment97 and delayed healing in a case of rhegmatogenous retinal detachment with multiple tears following surgical repair.98
In conclusion, tyrosine kinase inhibitors are promising treatments for a multi-targeted approach to retinal disease. Targeting multiple receptors, and thus affecting common downstream responses, as well as their various sustained-release formulations can prove effective in prolonging the therapeutic effect and decreasing treatment burden in, among other diseases, exudative AMD, DME and retinal vein occlusion.
Dr. Bou Said was a medical retina fellow at Mayo Clinic in Rochester when the article was written. Dr. Xu is an ophthalmology resident at the Mayo Clinic in Rochester. Dr. Bakri is Chair and Professor, Department of Ophthalmology, at the Mayo Clinic in Rochester.
1. Penn, J. S. et al. Vascular Endothelial Growth Factor in Eye Disease. Prog. Retin. Eye Res. 27, 331–371 (2008).
2. Witmer, A. N., Vrensen, G. F. J. M., Van Noorden, C. J. F. & Schlingemann, R. O. Vascular endothelial growth factors and angiogenesis in eye disease. Prog. Retin. Eye Res. 22, 1–29 (2003).
3. Yancopoulos, G. D. et al. Vascular-specific growth factors and blood vessel formation. Nature 407, 242–248 (2000).
4. Aiello, L. P. et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N. Engl. J. Med. 331, 1480–1487 (1994).
5. Whitescarver, T. D. et al. A History of Anti-VEGF Inhibitors in the Ophthalmic Literature: A Bibliographic Review. J. Vitreoretin. Dis. 5, 304–312 (2020).
6. Doggrell, S. A. Pegaptanib: the first antiangiogenic agent approved for neovascular macular degeneration. Expert Opin. Pharmacother. 6, 1421–1423 (2005).
7. Skelly, A., Bezlyak, V., Liew, G., Kap, E. & Sagkriotis, A. Treat and Extend Treatment Interval Patterns with Anti-VEGF Therapy in nAMD Patients. Vision 3, 41 (2019).
8. Arnold, J. J. et al. Two-year outcomes of ‘treat and extend’ intravitreal therapy for neovascular age-related macular degeneration. Ophthalmology 122, 1212–1219 (2015).
9. Rayess, N., Houston, S. K. S., Gupta, O. P., Ho, A. C. & Regillo, C. D. Treatment outcomes after 3 years in neovascular age-related macular degeneration using a treat-and-extend regimen. Am. J. Ophthalmol. 159, 3-8.e1 (2015).
10. Kelkar, A. et al. Factors affecting compliance to intravitreal anti-vascular endothelial growth factor therapy in Indian patients with retinal vein occlusion, age-related macular degeneration, and diabetic macular edema. Indian J. Ophthalmol. 68, 2143–2147 (2020).
11. Cox, J. T., Eliott, D. & Sobrin, L. Inflammatory Complications of Intravitreal Anti-VEGF Injections. J. Clin. Med. 10, 981 (2021).
12. Ghasemi Falavarjani, K. & Nguyen, Q. D. Adverse events and complications associated with intravitreal injection of anti-VEGF agents: a review of literature. Eye 27, 787–794 (2013).
13. Seah, I. et al. Use of biomaterials for sustained delivery of anti-VEGF to treat retinal diseases. Eye 34, 1341–1356 (2020).
14. Ranade, S. V. et al. The Port Delivery System with ranibizumab: a new paradigm for long-acting retinal drug delivery. Drug Deliv. 29, 1326–1334.
15. Sharma, A. et al. Port delivery system with ranibizumab (Susvimo) recall- What does it mean to the retina specialists. Int. J. Retina Vitr. 9, 6 (2023).
16. Chen, P.-H., Chen, X. & He, X. Platelet-derived growth factors and their receptors: structural and functional perspectives. Biochim. Biophys. Acta 1834, 2176–2186 (2013).
17. Guo, P. et al. Platelet-Derived Growth Factor-B Enhances Glioma Angiogenesis by Stimulating Vascular Endothelial Growth Factor Expression in Tumor Endothelia and by Promoting Pericyte Recruitment. Am. J. Pathol. 162, 1083–1093 (2003).
18. Carmeliet, P. & Jain, R. K. Molecular mechanisms and clinical applications of angiogenesis. Nature 473, 298–307 (2011).
19. Mitchell, T. S., Bradley, J., Robinson, G. S., Shima, D. T. & Ng, Y.-S. RGS5 expression is a quantitative measure of pericyte coverage of blood vessels. Angiogenesis 11, 141–151 (2008).
20. Jaffe, G. J. et al. Dual Antagonism of PDGF and VEGF in Neovascular Age-Related Macular Degeneration: A Phase IIb, Multicenter, Randomized Controlled Trial. Ophthalmology 124, 224–234 (2017).
21. Sadiq, M. A. et al. Platelet derived growth factor inhibitors: A potential therapeutic approach for ocular neovascularization. Saudi J. Ophthalmol. 29, 287–291 (2015).
22. Akwii, R. G., Sajib, M. S., Zahra, F. T. & Mikelis, C. M. Role of Angiopoietin-2 in Vascular Physiology and Pathophysiology. Cells 8, 471 (2019).
23. Khanani, A. M. et al. Angiopoietins as Potential Targets in Management of Retinal Disease. Clin. Ophthalmol. Auckl. NZ 15, 3747–3755 (2021).
24. Heier, J. S. et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. The Lancet 399, 729–740 (2022).
25. Ohara, H. et al. Faricimab for Diabetic Macular Edema in Patients Refractory to Ranibizumab or Aflibercept. Med. Kaunas Lith. 59, 1125 (2023).
26. Shibuya, M. Vascular Endothelial Growth Factor (VEGF) and Its Receptor (VEGFR) Signaling in Angiogenesis. Genes Cancer 2, 1097–1105 (2011).
27. Kim, K. & Khang, D. Past, Present, and Future of Anticancer Nanomedicine. Int. J. Nanomedicine 15, 5719–5743 (2020).
28. Terman, B. I. et al. Identification of the KDR tyrosine kinase as a receptor for vascular endothelial cell growth factor. Biochem. Biophys. Res. Commun. 187, 1579–1586 (1992).
29. Huang, L., Jiang, S. & Shi, Y. Tyrosine kinase inhibitors for solid tumors in the past 20 years (2001–2020). J. Hematol. Oncol.J Hematol Oncol 13, 143 (2020).
30. Carmeliet, P. et al. Synergism between vascular endothelial growth factor and placental growth factor contributes to angiogenesis and plasma extravasation in pathological conditions. Nat. Med. 7, 575–583 (2001).
31. Joussen, A. M. et al. Angiopoietin/Tie2 signalling and its role in retinal and choroidal vascular diseases: a review of preclinical data. Eye Lond. Engl. 35, 1305–1316 (2021).
32. Yu, X. et al. Suppression of KSHV-induced angiopoietin-2 inhibits angiogenesis, infiltration of inflammatory cells, and tumor growth. Cell Cycle Georget. Tex 15, 2053–2065 (2016).
33. J, O. et al. Suppression of angiogenesis and tumor growth by selective inhibition of angiopoietin-2. Cancer Cell 6, (2004).
34. Cross, M. J. & Claesson-Welsh, L. FGF and VEGF function in angiogenesis: signalling pathways, biological responses and therapeutic inhibition. Trends Pharmacol. Sci. 22, 201–207 (2001).
35. Casanovas, O., Hicklin, D. J., Bergers, G. & Hanahan, D. Drug resistance by evasion of antiangiogenic targeting of VEGF signaling in late-stage pancreatic islet tumors. Cancer Cell 8, 299–309 (2005).
36. Jeon, J., Sparreboom, A. & Baker, S. Kinase Inhibitors: the Reality Behind the Success. Clin. Pharmacol. Ther. 102, 726–730 (2017).
37. Bergers, G., Song, S., Meyer-Morse, N., Bergsland, E. & Hanahan, D. Benefits of targeting both pericytes and endothelial cells in the tumor vasculature with kinase inhibitors. J. Clin. Invest. 111, 1287–1295 (2003).
38. Bakri, S. J., Lynch, J., Howard-Sparks, M., Saint-Juste, S. & Saim, S. Vorolanib, sunitinib, and axitinib: A comparative study of vascular endothelial growth factor receptor inhibitors and their anti-angiogenic effects. PloS One 19, e0304782 (2024).
39. Jiang, H. et al. The multikinase inhibitor axitinib in the treatment of advanced hepatocellular carcinoma: the current clinical applications and the molecular mechanisms. Front. Immunol. 14, 1163967 (2023).
40. Hu-Lowe, D. D. et al. Nonclinical antiangiogenesis and antitumor activities of axitinib (AG-013736), an oral, potent, and selective inhibitor of vascular endothelial growth factor receptor tyrosine kinases 1, 2, 3. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 14, 7272–7283 (2008).
41. Moshfeghi, A. A. et al. U.S. Phase 1 Study of Intravitreal Axitinib Implant (OTX-TKI) for Neovascular Age-related Macular Degeneration. Invest. Ophthalmol. Vis. Sci. 64, 936 (2023).
42. Ocular Therapeutix, Inc. A Prospective Multicenter, Double-Masked, Randomized, Parallel-Group, Study to Evaluate the Safety, Tolerability, and Efficacy of OTX-TKI (Axitinib Implant) for Intravitreal Use in Subjects With Neovascular Age-Related Macular Degeneration (nAMD). https://clinicaltrials.gov/study/NCT04989699 (2024).
43. Ocular Therapeutix, Inc. A Phase 3, Multicenter, Double-Masked, Randomized, Parallel-Group Study to Evaluate the Efficacy and Safety of Intravitreal OTX-TKI (Axitinib Implant) in Subjects With Neovascular Age-Related Macular Degeneration (nAMD). https://clinicaltrials.gov/study/NCT06223958 (2024).
44. Ocular Therapeutix, Inc. A Phase 1B, Multicenter, Double-Masked, Randomized, Parallel Group Study to Evaluate the Safety, Tolerability, and Efficacy of OTX-TKI (Axitinib Implant) for Intravitreal Injection in Subjects With Moderately Severe to Severe Non-Proliferative Diabetic Retinopathy. https://clinicaltrials.gov/study/NCT05695417 (2023).
45. Clearside Biomedical, Inc. OASIS: Open-Label, Dose-Escalation, Phase 1/2a Study of the Safety and Tolerability of Suprachoroidally Administered CLS-AX Following Intravitreal Anti-VEGF Therapy in Subjects With Neovascular Age-Related Macular Degeneration. https://clinicaltrials.gov/study/NCT04626128 (2023).
46. Clearside Biomedical, Inc. ODYSSEY: A Phase 2b Study of Suprachoroidally Administered CLS-AX in Participants With Neovascular Age-Related Macular Degeneration. https://clinicaltrials.gov/study/NCT05891548 (2023).
47. Patel, S. R., Lin, A. S. P., Edelhauser, H. F. & Prausnitz, M. R. Suprachoroidal drug delivery to the back of the eye using hollow microneedles. Pharm. Res. 28, 166–176 (2011).
48. Marcus, D. M. et al. Safety and Tolerability Study of Suprachoroidal Injection CLS-AX in Neovascular AMD Patients with Persistent Activity Following Anti-VEGF Therapy (OASIS, NCT04626128; Extension Study NCT NCT05131646). Invest. Ophthalmol. Vis. Sci. 64, 728 (2023).
49. Clearside Biomedical, Inc. Extension Study to Evaluate the Long-Term Outcomes of Subjects Following CLS-AX Administration for Age-Related Macular Degeneration in the CLS-AX CLS1002-101 Study. https://clinicaltrials.gov/study/NCT05131646 (2023).
50. Schmid, T. A. & Gore, M. E. Sunitinib in the treatment of metastatic renal cell carcinoma. Ther. Adv. Urol. 8, 348–371 (2016).
51. Mulet-Margalef, N. & Garcia-del-Muro, X. Sunitinib in the treatment of gastrointestinal stromal tumor: patient selection and perspectives. OncoTargets Ther. 9, 7573–7582 (2016).
52. Raymond Eric et al. Sunitinib Malate for the Treatment of Pancreatic Neuroendocrine Tumors. N. Engl. J. Med. 364, 501–513 (2011).
53. Tanday, S. Sunitinib benefits patients with small-cell lung cancer. Lancet Oncol. 16, e164 (2015).
54. Yang, M. et al. GB-102 for Wet AMD: A Novel Injectable Formulation that Safely Delivers Active Levels of Sunitinib to the Retina and RPE/Choroid for Over Four Months. Invest. Ophthalmol. Vis. Sci. 57, 5037 (2016).
55. Peterson, W. et al. Ocular metabolism and melanin binding properties of sunitinib, a dual VEGFR/PDGFR inhibitor, that can safely prolong its efficacy for the treatment of wet AMD. Invest. Ophthalmol. Vis. Sci. 58, 1974 (2017).
56. Tsujinaka, H. et al. Sustained treatment of retinal vascular diseases with self-aggregating sunitinib microparticles. Nat. Commun. 11, 694 (2020).
57. Sharma, S. M. et al. Sunitinib Malate Preserves Retinal Ganglion Cells in Rodent NAION. Invest. Ophthalmol. Vis. Sci. 52, 6614 (2011).
58. Graybug Vision. A Phase 1/2 Multicenter Study Evaluating the Safety, Tolerability, and Efficacy of an Intravitreal Depot Formulation of Sunitinib Malate (GB-102) in Subjects With Neovascular Age-Related Macular Degeneration. https://clinicaltrials.gov/study/NCT03249740 (2019).
59. Graybug Vision. A Phase 2b Multicenter Dose-Ranging Study Evaluating the Safety and Efficacy of Sunitinib Malate Depot Formulation (GB-102) Compared to Aflibercept in Subjects With Neovascular (Wet) Age-Related Macular Degeneration (ALTISSIMO Study). https://clinicaltrials.gov/study/NCT03953079 (2022).
60. Hussain, R. M., Shaukat, B. A., Ciulla, L. M., Berrocal, A. M. & Sridhar, J. Vascular Endothelial Growth Factor Antagonists: Promising Players in the Treatment of Neovascular Age-Related Macular Degeneration. Drug Des. Devel. Ther. 15, 2653–2665 (2021).
61. Graybug Vision Reports Full Data Analysis After One Year Treatment Of GB-102 In Wet AMD. Yahoo Finance https://finance.yahoo.com/news/graybug-vision-reports-full-data-135016584.html (2021).
62. https://fyra.io. Graybug Vision Reports Analysis of Data from the 6-Month Extension Study of the ALTISSIMO Phase 2b Trial in Wet AMD. Eyewire+ https://eyewire.news/news/graybug-vision-reports-analysis-of-data-from-the-6-month-extension-study-of-the-altissimo-phase-2b-trial-in-wet-amd.
63. Yu, Y. et al. Sunitinib-Loaded Injectable Polymer Depot Formulation for Potential Once per Year Treatment of Neovascular Age-related Macular Degeneration (wet AMD). Invest. Ophthalmol. Vis. Sci. 59, 221 (2018).
64. Bendell, J. et al. A phase I trial of vorolanib (X-82t vascular endothelial growth factor receptor (VEGFR) inhibitor, in patients (pts) with advanced solid tumors. Ann. Oncol. 29, viii659–viii660 (2018).
65. Beckermann, K. E. et al. A Phase 1/2 Study to Evaluate the Safety and Activity of Nivolumab in Combination With Vorolanib, a Vascular Endothelial Growth Factor Tyrosine Kinase Inhibitor, in Patients With Refractory Thoracic Tumors. JTO Clin. Res. Rep. 5, (2024).
66. Science and Technology. EyePoint Pharmaceuticals https://eyepointpharma.com/technology/.
67. Abbey, A. M. et al. The DAVIO trial: a phase 1, open-label, dose-escalation study of a single injection of EYP-1901 (vorolanib in Durasert® platform) demonstrating reduced treatment burden in wet age-related macular degeneration. Invest. Ophthalmol. Vis. Sci. 64, 931 (2023).
68. Patel, S. et al. Phase I DAVIO Trial: EYP-1901 Bioerodible, Sustained-Delivery Vorolanib Insert in Patients With Wet Age-Related Macular Degeneration. Ophthalmol. Sci. 4, 100527 (2024).
69. EyePoint Pharmaceuticals, Inc. A Phase 1, Multicenter, Prospective, Open-Label, Dose Escalation Study of EYP-1901, a Tyrosine Kinase Inhibitor (TKI), in Subjects With Wet AMD. https://clinicaltrials.gov/study/NCT04747197 (2023).
70. EyePoint Pharmaceuticals, Inc. A Phase 2, Multicenter, Prospective, Randomized, Double-Masked, Parallel Study of EYP-1901, a Tyrosine Kinase Inhibitor (TKI), Compared to Aflibercept in Subjects With Wet AMD. https://clinicaltrials.gov/study/NCT05381948 (2024).
71. EyePoint Pharmaceuticals, Inc. A Phase 2, Multicenter, Prospective, Double-Masked, Parallel Study of EYP-1901, a Tyrosine Kinase Inhibitor (TKI), Compared to Sham for the Improvement of Moderately Severe to Severe Nonproliferative Diabetic Retinopathy (NPDR). https://clinicaltrials.gov/study/NCT05383209 (2024).
72. EyePoint Pharmaceuticals, Inc. A Phase 2, Multicenter, Prospective, Randomized, Double-Masked, Parallel Study of EYP-1901, a Tyrosine Kinase Inhibitor (TKI), Compared to Aflibercept in Subjects With Diabetic Macular Edema (DME). https://clinicaltrials.gov/study/NCT06099184 (2023).
73. EyePoint Pharmaceuticals Announces Positive Topline Data from the Phase 2 DAVIO 2 Trial of EYP-1901 in Wet AMD Achieving All Primary and Secondary Endpoints | EyePoint Pharmaceuticals. https://investors.eyepointpharma.com/news-releases/news-release-details/eyepoint-pharmaceuticals-announces-positive-topline-data-phase-2.
74. Howard-Sparks, M. et al. Neuroprotective effect of tyrosine kinase inhibitor vorolanib in a mouse model of retinal detachment. Invest. Ophthalmol. Vis. Sci. 64, 2829 (2023).
75. Shen, G. et al. Anlotinib: a novel multi-targeting tyrosine kinase inhibitor in clinical development. J. Hematol. Oncol.J Hematol Oncol 11, 120 (2018).
76. Lu, C. et al. A small molecular multi-targeting tyrosine kinase inhibitor, anlotinib, inhibits pathological ocular neovascularization. Biomed. Pharmacother. 138, 111493 (2021).
77. Kim, K.-H., Oh, J. Y., Cho, D. & Kim, M. J. J. Toward a Non-Invasive Solution of Wet AMD: Sunitinib, Pazopanib, and Axitinib Eyedrops versus Intraocular Injection of Aflibercept. Invest. Ophthalmol. Vis. Sci. 62, 447 (2021).
78. Ettrich, T. J. & Seufferlein, T. Regorafenib. Recent Results Cancer Res. Fortschritte Krebsforsch. Progres Dans Rech. Sur Cancer 211, 45–56 (2018).
79. Bayer. A Combined Phase IIa / IIb Study of the Efficacy, Safety, and Tolerability of Repeated Topical Doses of Regorafenib Eye Drops, in Treatment-Naïve Subjects With Neovascular Age Related Macular Degeneration. https://clinicaltrials.gov/study/NCT02222207 (2016).
80. Joussen, A. M. et al. The Developing Regorafenib Eye drops for neovascular Age-related Macular degeneration (DREAM) study: an open-label phase II trial. Br. J. Clin. Pharmacol. 85, 347–355 (2019).
81. Yafai, Y. et al. Anti-angiogenic effects of the receptor tyrosine kinase inhibitor, pazopanib, on choroidal neovascularization in rats. Eur. J. Pharmacol. 666, 12–18 (2011).
82. Singh, R. et al. Clinical evaluation of pazopanib eye drops in healthy subjects and in subjects with neovascular age-related macular degeneration. Retina Phila. Pa 34, 1787–1795 (2014).
83. GlaxoSmithKline. An Open-Label, Phase 2a Study to Evaluate Pazopanib Eye Drops Administered for 12 Weeks to Patients With Neovascular Age-Related Macular Degeneration. https://clinicaltrials.gov/study/NCT01362348 (2017).
84. Csaky, K. G. et al. Clinical evaluation of pazopanib eye drops versus ranibizumab intravitreal injections in subjects with neovascular age-related macular degeneration. Ophthalmology 122, 579–588 (2015).
85. Pick, A. M. & Nystrom, K. K. Pazopanib for the Treatment of Metastatic Renal Cell Carcinoma. Clin. Ther. 34, 511–520 (2012).
86. McLaughlin, M. M. et al. Initial exploration of oral pazopanib in healthy participants and patients with age-related macular degeneration. JAMA Ophthalmol. 131, 1595–1601 (2013).
87. GlaxoSmithKline. A Two-Part Study to Evaluate the Safety, Tolerability and Pharmacokinetics of Single and Repeat Oral Doses of Pazopanib in Healthy Adult Subjects. https://clinicaltrials.gov/study/NCT01051700 (2017).
88. GlaxoSmithKline. An Open-Label Pilot Study to Evaluate the Safety, Tolerability,Pharmacokinetics, Exploratory Efficacy and Pharmacodynamics of Oral Pazopanib Administered for 28 Days to Neovascular Age-Relatedmacular Degeneration Patients. https://clinicaltrials.gov/study/NCT01154062 (2017).
89. Tyrogenex. A Phase 1 Open-Label, Dose Escalation Clinical Trial to Evaluate the Safety and Preliminary Biologic Activity/Efficacy of the VEGFR/PDGFR Inhibitor X-82 Administered Per Os in Subjects With Neovascular Age-Related Macular Degeneration (AMD). https://clinicaltrials.gov/study/NCT01674569 (2018).
90. Tyrogenex. A Randomized, Double-Masked, Placebo-Controlled, Dose- Finding, Non-Inferiority Study of X-82 Plus Prn Intravitreal (Ivt) Anti-VEGF Compared to Prn Ivt Anti-VEGF Monotherapy in Neovascular AMD. https://clinicaltrials.gov/study/NCT02348359 (2022).
91. AnewPharma. Phase I Study of CM082 in Patients With Myopic Choroidal Neovascularization (CNV). https://clinicaltrials.gov/study/NCT04222842 (2021).
92. AnewPharma. Phase 1 Study of CM082 in Patients With wAMD: Safety, Tolerability, Pharmacokinetics, and Preliminary Efficacy. https://clinicaltrials.gov/study/NCT02452385 (2020).
93. AnewPharma. Phase 2 Study of Intermittent Oral Dosing of CM082 in Patients With wAMD: Safety, Tolerability, Pharmacokinetics, and Preliminary Efficacy. https://clinicaltrials.gov/study/NCT03710863 (2020).
94. Jackson, T. L. et al. Oral Tyrosine Kinase Inhibitor for Neovascular Age-Related Macular Degeneration: A Phase 1 Dose-Escalation Study. JAMA Ophthalmol. 135, 761–767 (2017).
95. Gao, Y. et al. Safety and tolerability of oral vorolanib for neovascular (wet) age-related macular degeneration: a phase I, open-label study. Eye 37, 3228–3233 (2023).
96. Knickelbein, J. E. et al. Systemic Sunitinib Malate Treatment for Advanced Juxtapapillary Retinal Hemangioblastomas Associated with von Hippel-Lindau Disease. Ophthalmol. Retina 1, 181–187 (2017).
97. Wegner, A. & Khoramnia, R. Neurosensory retinal detachment due to sunitinib treatment. Eye 25, 1517–1518 (2011).
98. https://fyra.io. Watch For Retinal Findings With Systemic Pazopanib. Retina Today https://retinatoday.com/articles/2021-nov-dec/watch-for-retinal-findings-with-systemic-pazopanib.
99. Alshaikh, R. A., Waeber, C. & Ryan, K. B. Polymer based sustained drug delivery to the ocular posterior segment: barriers and future opportunities for the treatment of neovascular pathologies. Adv. Drug Deliv. Rev. 187, 114342 (2022).
100. Ocular Therapeutix, Inc. A Phase 1 Open-Label, Dose Escalation Study of OTX-TKI for Intravitreal Use in Subjects With Neovascular Age-Related Macular Degeneration (AMD). https://clinicaltrials.gov/study/NCT03630315 (2022).
101. Tan, C. S., Ngo, W. K., Chay, I. W., Ting, D. S. & Sadda, S. R. Neovascular Age-Related Macular Degeneration (nAMD): A Review of Emerging Treatment Options. Clin. Ophthalmol. Auckl. NZ 16, 917–933 (2022).
102. Graybug Vision. A Phase 2a Multicenter Study Evaluating the Safety, Tolerability, and Pharmacodynamics of Sunitinib Malate Depot Formulation (GB-102) in Subjects With Diabetic Macular Edema (DME) and Retinal Vein Occlusion (RVO). https://clinicaltrials.gov/study/NCT04085341 (2021).


