The Calhoun Vision Light-adjustable Lens is one of the more eagerly anticipated technologies in ophthalmology, holding out the hope of being able to adjust a patient’s intraocular lens postoperatively in response to any residual refractive error. As the LAL investigations for postop adjustments proceeded, however, researchers discovered that the adjustment process might also be able to craft a lens that could go beyond correcting refractive “surprises” and actually treat presbyopia. With the lens poised to enter its Phase III trial in the United States, here’s a look at the technology and how it’s performing as a presbyopic treatment.
Making the Adjustment
The LAL is a silicone lens with two C-PMMA haptics. However, the silicone macromers that are homogeneously distributed throughout the lens are photosensitive to the near-ultraviolet wavelength of energy. As such, when energy of this wavelength strikes the lens in specific patterns, it changes the distribution of the macromers and, subsequently, the refractive power of the lens. To induce a myopic adjustment, for instance, the pattern puts more energy in the periphery of the lens, and vice versa for a hyperopic adjustment. A cylindrical adjustment is also possible. Once the surgeon feels the lens has been made as accurate as possible, a final irradiation step locks in the power change. According to Arturo Chayet, MD, who practices in Tijuana, Mexico, and has worked with the lens, the range of correction is ±2 D for sphere and 2.5 D for astigmatism at the spectacle plane.
In terms of results, a recent prospective study looked at 122 cataract patients receiving the LAL. Their pre-adjustment residual errors of 0.96 ±0.85 D of sphere and -0.98 ±0.5 D of cylinder were corrected and remained stable for 18 months of follow-up, the surgeons say. Post-adjustment, 100 percent of the patients were within 0.5 D of emmetropia, with an average final refraction of 0.03 ±0.17 D.1
Addressing Presbyopia
Surgeons working with the lens say it offers three approaches to presbyopia.
“The first approach is monovision,” says Dr. Chayet. “In general, for a patient to be satisfied with monovision, you really need to get the dominant eye to 20/20 for distance, and I think this technology gives you the best chance to do this. You then have to adjust the lens so the non-dominant eye is -1 D, and the patient then has about two to three weeks to see if he likes it before locking it in. If he doesn’t like it, we can bring the eye to emmetropia with an adjustment.
“The second presbyopia solution is the so-called customized near add,” Dr. Chayet continues. “With the CNA, you set the dominant eye for distance, but then customize the non-dominant eye based on the patient’s visual needs and occupation. You can also customize it to the size of the pupil. For instance, in some cases, a patient may have smaller mesopic pupils, so you should then do a smaller treatment, making sure that he’s got most of the near vision at all times. You just change the size of the treatment zone.”
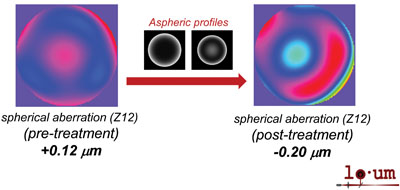
The third approach to presbyopia available to the LAL is a customized aspheric treatment, and makes more use of the near-ultraviolet illumination’s ability to fine-tune the shape of the lens. Pablo Artal, PhD, of the University of Murcia in Spain, helped develop the light patterns used with the LAL, including the aspheric treatment. He says the surgeon he works with, Jose Maria Marin, MD, has performed 50 aspheric treatments on presbyopes to date. “With a clever type of irradiation profile, you can induce aberrations in the lens, including spherical aberration,” Dr. Artal explains. “It’s well-known that if you induce spherical aberration in any optical system, you increase the depth of focus and, as a consequence, you get some intermediate or near vision. Typically, this involves a compromise where the distance vision is reduced a little. The good thing with the adjustable lens, though, is you can select the amount of spherical aberration for a particular patient. So, you can explore this with the patient before treatment.
“We use a prototype of an instrument called the Rapid Optics Analyzer [Voptica],” Dr. Artal adds. “The ROA allows the patient to experience the same amount of spherical aberration as he’d receive in the lens and say whether he likes it or not. We basically ask the patient to select the amount of spherical aberration he’d be comfortable with. Once we get this value, this is our target for the adjustable lens.” In practice, one eye is usually optimized for distance vision while the other gets the spherical aberration profile. “So, it’s a type of modified monovision in a way,” says Dr. Artal. He says the average spherical aberration target for the presbyopes who have received this treatment is -0.12 µm for a 4-mm pupil. “Though there is some variability, of course, most patients maintain 20/20 distance acuity,” Dr. Artal says. “For near vision, at 40 cm most get J1, a very typical result. At 30 cm, maybe J2 or worse, and then J1+ for 60 cm, all measured binocularly.”
|
“We didn’t measure stereoacuity very systematically,” Dr. Artal continues. “But it would involve more or less the same type of stereoacuity issues as you’d find in a micro-monovision type of surgery. Here, it’s a little bit less than in micro-monovision because the disparity between the two images is smaller. We haven’t had any major complaints from patients so far.
Finally, the timing of the procedures has the potential to be a challenge for some patients. “The process is, first, you do the standard surgery, then wait about 10 days to two weeks,” explains Dr. Artal. “Then you go through the first light adjustment to correct sphere and cylinder. You can then eventually have a second adjustment to those values to refine them. However, if they’re OK, you can just have the secondary aspheric adjustment. That’s one of the main practical issues of this technology.
“Though I like it very much and see a lot of potential, one of the problems right now is, for one eye you need at least four visits for treatment in addition to the standard surgery, so it’s kind of demanding,” adds Dr. Artal. “Patients also have to wear sunglasses for about three weeks during the process, sometimes longer. And, in order to get good results, it’s not only about the treatment, but you need to do a good job with all the refractive analyses. If you get an inaccurate initial refraction, everything is going to be wrong. Calhoun Vision is trying to reduce the process to one lock-in step instead of two, which should eliminate one visit, since up until now we’ve been doing two light treatments and two lock-ins. However, I don’t think it would be possible to reduce it to less than three if you’re also doing an aspheric treatment. Of course, if you’re only doing a refractive correction, then you can have two visits—one light treatment and one lock-in. That would be the minimum.” REVIEW
Drs. Chayet and Artal are consultants to Calhoun Vision, and Dr. Artal is the founder of Voptica.
1. Hengerer F, Dick H, Conrad-Hengerer I. Clinical evaluation of an ultraviolet light adjustable intraocular lens implanted after cataract removal. Ophthalmology 2011;118:12:2382-8.