It’s always interesting to see how new intraocular lens technology fares as it tries to capture the interest of cataract surgeons. Physicians often take a watchful-waiting approach, ensuring that a new lens has the efficacy and safety profile they want before incorporating it into their everyday practice. This seems to be the case with the most recent additions to the premium IOL market, the Vivity (Alcon) and the Synergy (Johnson & Johnson Vision), though a fair number of respondents on this year’s IOL survey have begun using them in patients already.
This is just one of the findings from this year’s e-mail survey on IOL preferences. This time around, 22 percent of the 11,518 recipients on Review’s e-mail list opened the message, and 54 surgeons took the survey.
To read about your colleagues’ impressions of the newcomers on the IOL scene, as well as other lens technologies, read on.
 |
Premium Preferences
Surgeons who implant premium intraocular lenses are embracing technology such as trifocal IOLs, but are also warming up to the latest additions to the market.
The most popular premium lens option among the respondents (with some surgeons choosing more than one option) is the PanOptix Trifocal (non-toric), with 54 percent of the respondents saying they implant it (average number implanted per month: 8; average charge/eye: $2,705). Following the non-toric PanOptix was its toric counterpart, used by 46 percent of the physicians (average number implanted per month: 7; average charge/eye: $2,783).
A New York surgeon says he uses the PanOptix due to “less haloes and a crisper quality of vision.” Another New York surgeon says he chooses the PanOptix because of “Excellent distance and near, with tolerable night distractions.”
“[The PanOptix has] less dysphotopsia, more near vision, and is less dependent on ocular surface,” says a surgeon from Cincinnati.
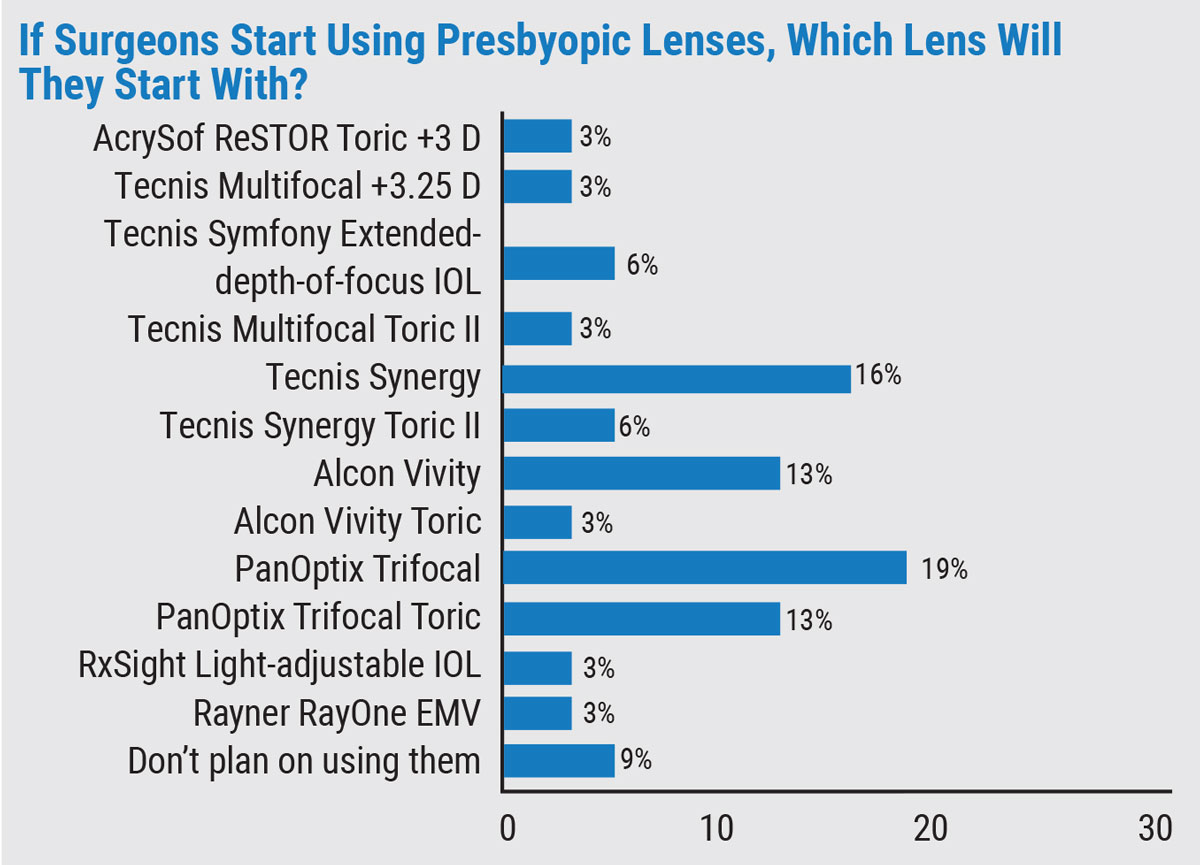
The next most popular group of premium lenses are the most recently approved ones, the Alcon Vivity and J&J Vision Tecnis Synergy lens families. The Vivity is a non-diffractive, extended-depth-of-focus IOL with a unique central optic zone. The Synergy has been described as a kind of mix between the Symfony and the Tecnis multifocal, since it combines elements of an EDOF lens with a diffractive multifocal to provide a range of vision.
Thirty-three percent of surgeons say they implant the non-toric Vivity (average number implanted per month: 7; average charge/eye: $2,524), and 24 percent implant the toric version (average number implanted per month: 6; average charge/eye: $2,911). Twenty-six percent of the surgeons on the survey implant the Tecnis Synergy (average number implanted per month: 9; average charge/eye: $2,656), and 22 percent implant the Tecnis Synergy Toric II (average number implanted per month: 6; average charge/eye: $2,599). Fifteen percent implant the original Symfony EDOF Toric II lens (average number implanted per month: 3; average charge/eye: $2,324).
 |
A Los Angeles surgeon says, “Vivity is my favorite premium IOL because it gives an improved range of focus, largely without night driving glare problems.”
New York’s James Hu, MD, a Vivity user, likes the lens, but sees some room for improvement. “I get issues with late decentration; day one postop and one week postop, the IOL will be perfectly centered around the pupil, but at a month I’ve noticed the IOL will shift 0.5 mm (usually inferotemporal or superotemporal), despite following most of the pearls for IOL centration.”
Oklahoma City ophthalmologist Deena Sylvester says, “I like that the Vivity doesn’t have halos/glare, but I wish it could provide better 14- to 16-inch reading.”
Colorado Springs surgeon Steve Dewey likes using the J&J Tecnis MF Toric II and the new Synergy. “I have to target appropriate refractive error, usually +0.25 D sphere. The J&J lenses give great contrast, amazing acuity and a fantastic range [of vision].”
 |
Only 23 percent of the surgeons say they mix IOLs to give patients a greater depth of focus.
Dr. Dewey says he mixes-and-matches with the Symfony and the +3.25 Tecnis MF IOL, and includes the toric versions as necessary. “Mixing-and-matching is suitable for mild ocular pathologies (asymptomatic epiretinal membrane, presence of a few drusen, treatable dry eye),” he says, “knowing that we can’t always predict the result of the surgery in light of minor pathologies. Otherwise, in a ‘perfect’ eye, Synergy bilaterally works great.”
Dr. Sylvester says, “Very rarely do I mix-and-match. If the first eye with a Vivity isn’t satisfactory enough for the patient at near, I’ll consider PanOptix in the second eye. This has been good for the two patients I’ve done this in.”
A Cincinnati surgeon says he doesn’t mix-and-match because, “I’m nervous about patients noting subtle differences between their eyes.”
Monofocal Mainstays
Surgeons also opined about the lenses they use for the bulk of their patients.
The Alcon IQ Aspheric was the single most popular choice, chosen by 37 percent of the respondents. The J&J Tecnis 1-piece was next, with 20 percent of the respondents preferring it. Twelve percent say they often use the new Tecnis Eyhance, and 8 percent prefer the B+L enVista.
A surgeon from Georgia who uses the Alcon lens says, “I like the gentle opening in the bag. I dislike the 6-mm optic (would prefer 7-mm), the lack of a square edge for delaying PCO, and that the haptics don’t open enough or have enough spring for unassisted centering.”
Dr. Dewey uses the Tecnis 1-piece. “It yields good acuity, amazing contrast and is relatively forgiving with good acuity over a small range of refractive errors,” he says. A physician from New Orleans also uses the J&J lenses, and sees strengths and weaknesses in each. “I like the full range of vision with the Synergy,” he says. “I don’t like the nighttime glare. It’s the opposite with the Eyhance: It gives marginal near vision, but there are no complaints with night driving. I use more Eyhance than Synergy.”
A Kansas surgeon who prefers the enVista says he does so because “There are no glistenings, and it has a durable surface that won’t scratch.”
 |
Toric IOLs
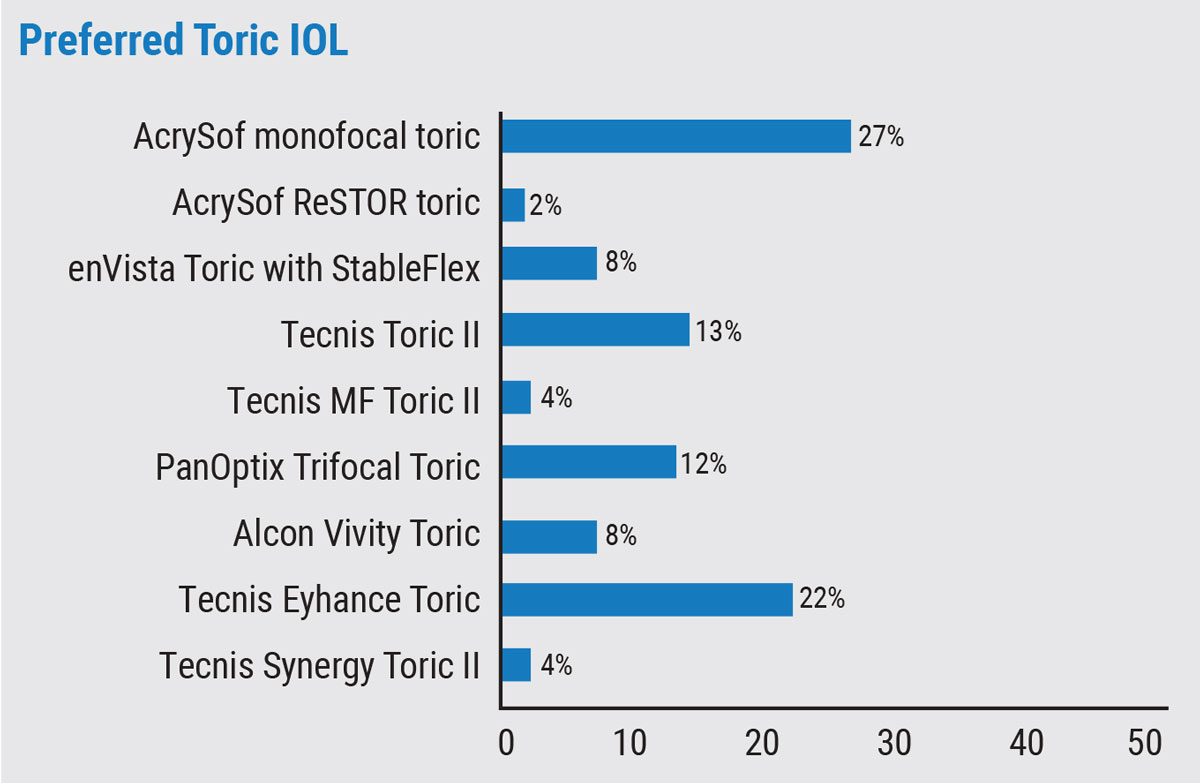
For tackling patients’ astigmatism with an IOL, the most popular option on the survey was the AcrySof monofocal toric (27 percent), followed by the Tecnis Eyhance toric (22 percent). Fourteen percent say they prefer the Tecnis Toric II and 12 percent like the PanOptix trifocal toric.
Robert Mobley, MD, of Clinton Township, Michigan, says that he likes the AcrySof monofocal toric for its “good stability and centration.” Colorado’s Dr. Dewey uses the new Eyhance. “I appreciate the enhanced range of the Eyhance, and I appreciate how the frosted haptics reduce post-implantation rotation,” he says.
 |
Phakic Lenses
Only a fifth of the respondents say they implant phakic IOLs, with the majority of them (91 percent) preferring to use the Visian toric or non-toric. The rest say they implant the Artiflex/Veriflex.
A Cincinnati surgeon who uses the Visian says, “It’s easy to insert, has great optics, and the material is easy to work with. Loading is challenging and looking forward to not having to create PIs [with the upcoming Visian EVO]. A surgeon from Los Angeles agrees, saying, “It’s a much better option than LVC, especially in moderate to super-high myopes if they’re sufficient candidates.” St. Louis’ Krishnarao Rednam says the Visian “gives good outcomes.”
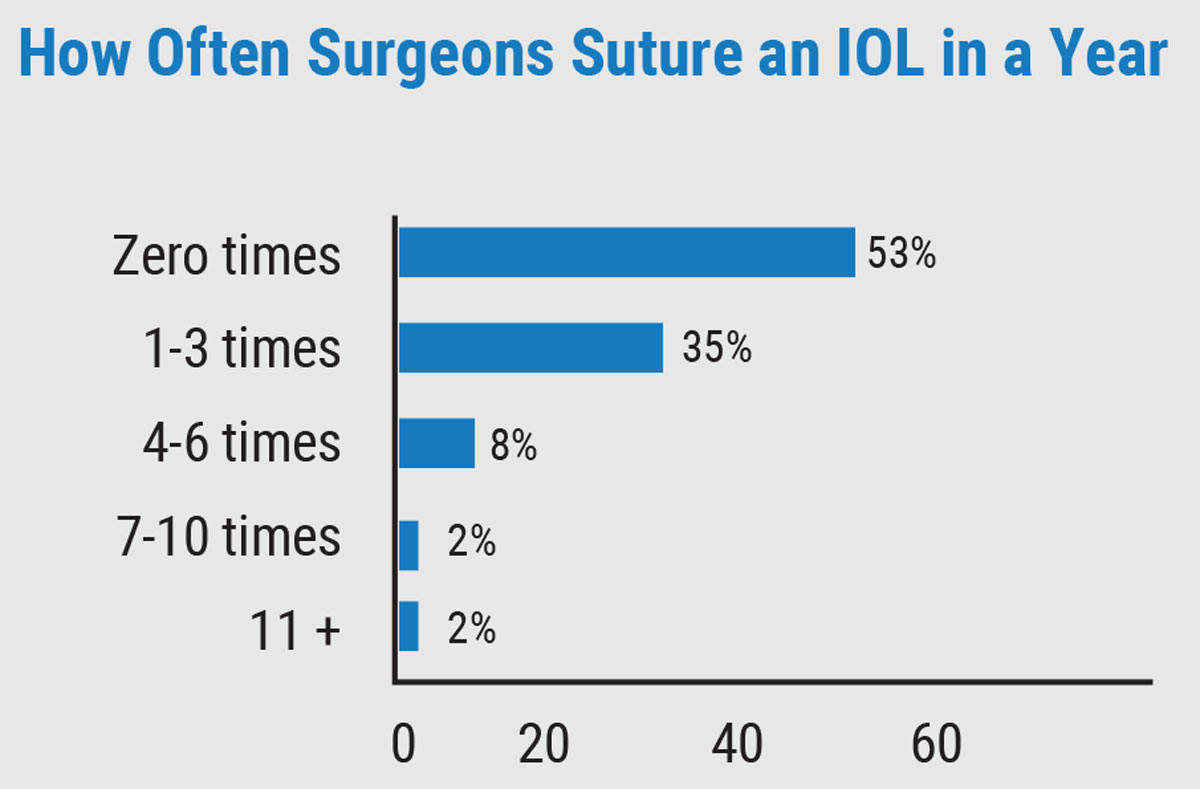
Suture Situations
The respondents also discussed suturing IOLs. Fifty-three percent say they usually don’t have to suture an IOL in any given year, and 35 percent say they find themselves suturing a lens one to three times in that span.
The main reasons given for suturing lenses:
- loss of zonular support due to pseudoexfoliation;
- late bag and lens dislocation;
- missing zonules; and
- immunosuppressed patients who are poor healers.
In the end, surgeons seem content with their lens options, but there’s a sense that the ideal premium lens has yet to arrive. Says Minneapolis surgeon Jesse Dovich, MD, “We need a fully accommodative IOL.”
This article has no commercial sponsorship.