Over the past six years, we have made great progress in understanding the complex genetics underlying age-related macular degeneration. At this point more than 25 genes have been reported to influence AMD risk, and the identification of the major genetic risk factors has elucidated new therapeutic targets, such as the alternative complement pathway.1 This knowledge, combined with advances in technology allowing for rapid and precise genotyping, make it now possible to profile an individual’s genetic risk for AMD.
Genetic Tests for AMD Risk
There already are several commercially available tests for determining an individual’s genetic risk for AMD as listed in Table 1.
The various tests differ in the numbers of genetic markers and methods used for calculating risk. The two main tests currently directed to ophthalmic providers for patient risk stratification are Macula Risk (ArcticDx) and RetnaGene (Sequenom). The Macula Risk test uses markers in four genes as well as smoking history to predict an individual’s risk of advanced AMD and categorizes patients into five risk groups (one to five, with five representing highest risk). Sequenom’s RetnaGene test employs an independently validated model using 13 single nucleotide polymorphisms in the major AMD-associated genes and is geared specifically for predicting risk of the neovascular form of AMD. A risk score is generated and the patient is categorized into three risk groups: low; medium; or high. DeCODE genetics offers AMD risk screening as part of its Complete scan which analyzes genetic risk factors for 50 conditions and must be ordered through a physician. The 23andMe test is a retail product available directly to the general population.
|
The ACCE Model
Now that these tests are available, it is necessary to determine whether it is worthwhile to perform genetic testing. The Centers for Disease Control and Prevention sponsored the development of the ACCE model for evaluating scientific data on emerging genetic tests. This model considers four components: 1) analytic validity; 2) clinical validity; 3) clinical utility; and 4) ethical/legal/social implications.2
Analytic Validity
The criterion of analytic validity refers to the technical accuracy of the test. Current technology makes genotyping very accurate. Therefore, determining whether an individual has the high-risk or low-risk allele at a specific single nucleotide polymorphism is performed quite reliably. The main source of error with the current tests available would be likely due to problems with sample handling.
Clinical Validity
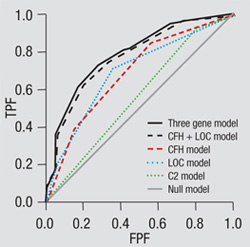
The measure of clinical validity asks how well a test can actually discriminate between high- and low-risk groups. A method for calculating this discriminative ability is plotting true positives vs. false positives, which is called a receiver operating curve (ROC) (See Figure 1).
The area under this curve (AUC) is a measure of discriminative ability, with a perfect test giving an AUC of one. The recommended AUC of a model for screening a population at increased risk of disease is >0.75.3 Current models for predicting AMD risk that include various combinations of epidemiologic, clinical and genetic factors give AUC’s of approximately 0.8.4,5,6 Therefore, these models appear to have sufficient accuracy for predicting advanced AMD in those already at increased risk based on age or evidence of early AMD.
|
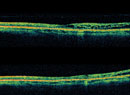
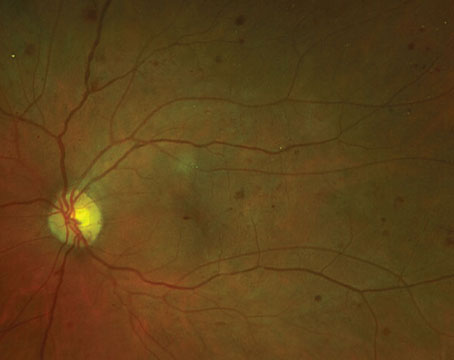
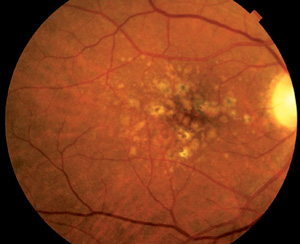
How much does genotyping add to our ability to predict advanced AMD? A previous analysis by Johanna Seddon, MD, and colleagues demonstrated that a model of AMD risk including age, gender, education, baseline AMD grade, smoking and body mass index had an AUC of 0.757.6 The addition of genetic factors (SNPs in CFH, ARMS2, C2, CFB and C3) increased the AUC to 0.821. In these models, the baseline grade of AMD was the strongest predictor of risk of progression to advanced AMD. More recently, work by Michael Klein, MD, et al. confirmed that an individual’s macular phenotype, represented by the AREDS Simple Scale score (See Table 2 and Figure 2), has the greatest predictive value.7 The predictive models in this analysis included age, family history, smoking, the AREDS Simple Scale score, the presence of very large drusen, the presence of advanced AMD in one eye, and two polymorphisms in CFH and ARMS2 strongly associated with risk of AMD. The AUC was 0.872 with genetic factors included and 0.865 without. These data indicate that it is possible to provide accurate assessment of risk of advanced AMD without necessarily doing genetic testing. The authors have made their risk calculator available online at
caseyamdcalc.ohsu.edu.
One other measure of clinical validity is positive predictive value (PPV) or the percentage of individuals identified as high-risk who will actually develop advanced disease. This value correlates with disease prevalence. With regard to the AMD scenario, the PPV of any genetic test will be better if applied to elderly individuals with early stages of AMD rather than young, unaffected individuals.
Clinical Utility
The measure of clinical utility considers how the test results will affect clinical management of the individual. What can we do for those individuals whose genetic testing indicates that they are at high risk for vision loss from AMD? Currently, we do not have preventive measures other than high-dose antioxidant and zinc supplements as demonstrated by the Age-Related Eye Disease Study.8 Experience from genetic testing for Alzheimer’s disease revealed that those who knew that they carried the risk variant in the ApoE gene reported that they were more likely to use dietary supplements as a preventive measure against the development of the disease.9 The same might hold true for those determined to be at high-risk for advanced AMD. However, some evidence suggests that those with the CFH Y402H risk allele might have a reduced benefit from taking the AREDS supplements.10
We might also suggest more frequent monitoring for high-risk patients and possibly recommend home monitoring devices. Preferential hyperacuity perimetry has been demonstrated to detect early neovascular AMD with high sensitivity and specificity.11,12 This technology has been developed for home monitoring, and other applications are being developed for smartphones and computers. The impact of recommending such monitoring for high-risk patients will need to be assessed.
What about using genetics to guide therapy? So far, there have been no consistent associations between response to anti-VEGF therapy and genotype.13-15 However, associations may emerge in the future as new therapeutic pathways are targeted, for example the complement pathway. Also, the studies to date have been performed to a limited number of polymorphisms. As genotyping technology continues to improve and becomes more affordable, more extensive analyses may be performed revealing new associations.
| ||||||||||||||||||||
Ethical/Legal/Social Implications
Currently there do not appear to be any particular ethical or social issues associated with genetic testing for AMD. As noted previously, genetic testing for AMD should only be considered for patients with early-stage disease and not for young, presymptomatic individuals. Therefore, the results of this testing should not necessarily label individuals with a new diagnosis. However, the impact of being predicted to be at high-risk of vision loss from AMD should not be underestimated and options for counseling should be available, as recommended for all other genetic testing.
Where We Stand Today
Should we offer genetic testing in routine clinical practice? In terms of the ACCE paradigm, the analytic validity of AMD genetic tests is good, meaning there are no technical difficulties in genotyping the major risk variants. Clinical validity is also good in terms of being able to accurately identify high-risk patients. However, we must keep in mind that the accuracy is highest if we apply these tests to those with early-stage disease rather than the general population. In terms of clinical utility, we are still exploring how the results of testing will be applied to the management of patients with AMD. At the present time, there do not appear to be significant ethical, legal and social implications of genetic testing for AMD, but these issues should be reassessed as utilization increases.
The most significant impact of the identification of genetic risk factors for AMD has been the insight provided regarding potential therapeutic targets as a result of the elucidation of pathways involved in disease pathogenesis. Genotyping will remain a critical element of ongoing and future clinical trials as more information regarding genetics and specific disease manifestations (genotype-phenotype correlations) as well as genetics and response to therapy (pharmacogenetics) remains to be discovered. Outside of the trial setting, given the growing availability of commercial genetic tests for AMD, clinicians will require some knowledge about these tests in order to have an informed discussion with patients who are interested in knowing their genetic profile. REVIEW
Dr. Kim is an associate professor of ophthalmology at the Harvard Medical School and on the Retina Service at Massachusetts Eye and Ear Infirmary. Contact her at (617) 573-3367; fax: (617) 573-3678 or
ivana_kim@meei.harvard.edu.
Figure 1 adapted from Jakobsdottir J et al. PLoS Genet. Feb;5(2):e1000337. Epub 2009 Feb 6. doi:10.1371/journal.pgen.1000337.g003.
1. DeAngelis MM, Silveira AC, Carr EA, Kim IK. Genetics of age-related macular degeneration: current concepts, future directions. Semin Ophthalmol 2011 May;26(3):77-93.
2. Centers for Disease Control and Prevention. ACCE. http://www.cdc.gov/genomics/gtesting/ACCE/FBR/index.htm
3. Janssens AC, Moonesinghe R, Yang Q, Steyerberg EW, et al. The impact of genotype frequencies on the clinical validity of genomic profiling for predicting common chronic diseases. Genet Med 2007;9:528-535.
4. Jakobsdottir J, Gorin MB, Conley YP, Ferrell RE, Weeks DE. Interpretation of genetic association studies: Markers with replicated highly significant odds ratios may be poor classifiers. PLoS Genet 2009 Feb;5(2):e1000337. Epub 2009 Feb 6.
5. Hageman GS, Gehrs K, Lejnine S, et al. Clinical validation of a genetic model to estimate the risk of developing choroidal neovascular age-related macular degeneration. Human Genomics 2011 July;5(5):1-21.
6. Seddon JM, Reynolds R, Maller J, Fagerness JA, et al. Pre-diction model for prevalence and incidence of advanced age-related macular degeneration based on genetic, demographic, and environmental variables. Invest Ophthalmol Vis Sci 2009 May;50(5):2044-53.
7. Klein ML, Francis PJ, Ferris FL 3rd, Hamon SC, Clemons TE. Risk assessment model for development of advanced age-related macular degeneration. Arch Ophthalmol 2011 Dec;129(12):1543-50. Epub 2011 Aug 8.
8. Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol 2001;119:1417-36.
9. Green RC, Roberts JS, Cupples LA, Relkin NR, et al; REVEAL Study Group. Disclosure of APOE genotype for risk of Alzheimer’s disease. N Engl J Med 2009 Jul 16;361(3):245-54.
10. Klein M, Francis P, Rosner B, et al. CFH and LOC387715/ARMS2 Genotypes and Treatment with Antioxidants and Zinc for Age-Re-lated Macular Degeneration. Ophthalmology 2008;115:1019-1025.
11. Alster Y, Bressler NM, Bressler SB, Brimacombe JA, et al; Preferential Hyperacuity Perimetry Research Group. Preferential Hyperacuity Perimeter (PreView PHP) for detecting choroidal neovascularization study. Ophthalmology 2005112:1758-65.
12. Lai Y, Grattan J, Shi Y, Young G, Muldrew A, Chakravarthy U. Functional and morphologic benefits in early detection of neovascular age-related macular degeneration using the preferential hyperacuity perimeter. Retina 2011;31:1620-6.
13. Lee AY, Raya AK, Kymes SM, Shiels A, Brantley MA Jr. Pharmacogenetics of complement factor H (Y402H) and treatment of exudative age-related macular degeneration with ranibizumab. Br J Ophthalmol 2009 May;93(5):610-3.
14. Kloeckener-Gruissem B, Barthelmes D, Labs S, Schindler C, Kurz-Levin M, Michels S, Fleischhauer J, Berger W, Sutter F, Menghini M. Genetic association with response to intravitreal ranibizumab (Lucentis) in neovascular AMD patients. Invest Ophthalmol Vis Sci 2011 Jul 1;52(7):4694-702.
15. McKibbin M, Ali M, Bansal S, Baxter PD, West K, Williams G, Cassidy F, Inglehearn CF. CFH, VEGF and HTRA1 promoter genotype may influence the response to intravitreal ranibizumab therapy for neovascular age-related macular degeneration. Br J Ophthalmol 2012 Feb;96(2):208-12.