Spontaneous globe subluxation is a rare orbital complication and presents in a dramatic fashion. It is characterized by the anterior displacement of the eye, usually when the equator of the globe protrudes beyond the retracted lids. Over the past century, fewer than 30 cases of spontaneous subluxation of the globe have been reported. When it presents it can be dramatic and produce anxiety for the patient and ophthalmologist. Because this is a fairly uncommon entity, this article will review the history and epidemiology, clinical characteristics and complications and, lastly, treatment options.
History
The first reported case of dislocation of the eye was in 1907.1 Several case reports have documented various presentations and treatments since then. In 2002, John C. Kunesh, MD, and Steven E. Katz, MD, reviewed all reported cases from 1907 to 2002, and they documented an age range from 11 months to 73 years with a mean age of 38 years. No sex predilection or specific racial distribution was found in this review of 26 cases.2
Clinical Presentation and Complications
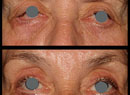
Clinically, globe subluxation can vary in presentation from asymptomatic to blindness secondary to traumatic optic neuropathy. The most common presentation is spontaneous subluxation after a precipitating trigger, usually eyelid manipulation by the physician or caregiver. One reported case of globe subluxation was even reported after placement of a soft contact lens (See image below).2 Beyond lid manipulation, patients can present with varying underlying risk factors such as exophthalmos, severe lid retraction, floppy eyelid syndrome, thyroid orbitopathy or conditions that predispose patients to shallow orbits such as Crouzon's syndrome. Myopia was shown not to be an independent risk factor. These risk factors are not absolute and certainly there seems to be an underlying unknown pathophysiological mechanism that gives these patients a higher probability of subluxation.
Globe subluxation can fall into three categories: spontaneous; voluntary; or traumatic. A review of the literature shows that of the reported cases, the majority are spontaneous.2 Spontaneous globe subluxation has been defined as occurring without conscious effort or without a precipitating factor. Voluntary globe subluxation is defined as the ability to express one's globe without any precipitating trigger. Traumatic globe subluxation occurs without conscious effort after direct trauma.
The pathophysiology of globe subluxation is unknown, but the mechanism is quite clear. Usually a patient or a caregiver will manually spread the eyelids, causing posterior pressure against the globe. In turn the globe advances, the cornea becomes dry, inducing a blink reflex. This causes contraction of the orbicularis muscle causing the eye to lock forward making digital manipulation and repositioning of the globe back in the orbit difficult.
Symptoms that result from subluxation can vary from asymptomatic, to pain to blurred vision. Other complications that have been reported include exposure keratopathy, corneal abrasion, blepharospasm and traumatic optic neuropathy. There is only one reported case of bilateral optic neuropathy secondary to voluntary globe luxation in a setting of floppy eyelid syndrome.3
Treatment
In the acute event, immediate reduction of the globe is paramount. Sometimes relaxing the patient, leaning the patient back in the chair is enough to reposition the globe in place. Topical anesthetic drops have been used to break the exposure/dry-eye cycle, allowing the physician to more easily digitally reposition the globe. David Tse, MD, has described two maneuvers to reposit a subluxed globe. First, while the patient maintains downward gaze, the upper eyelid is pulled upward and the globe is simultaneously depressed with the index finger of the other hand.5 The other method utilizes a small Desmarres retractor or a paper clip, spread at a right angle; this is introduced between the upper lid margin and superior rectus. Once the tip is under the eyelid, digital manipulation downward of the globe is necessary to reposit the globe. Once the eyelid is over the equator, the patient is instructed to look up pulling the eyelid over the eye. If difficulty is found with this technique, a supplemental facial nerve block can aid in relaxing the orbicularis muscle. In rare cases, conscious sedation and even general anesthesia may be necessary, especially in children and mentally handicapped individuals.
Prevention of further episodes begins with educating the patient on potential triggers, including lid manipulation. Patients with an underlying disease process such as thyroid orbitopathy should seek treatment of their disease, and they should be instructed on proper repositioning techniques. Surgical options include lateral tarsorrhaphy, lid retraction repair and bony or fatty orbital decompression in severe cases. The presence of underlying diseases like Grave's disease or a space-occupying orbital lesion causing autoproptosis should be identified before considering surgical interventions.
Drs. Takle and Murchison are in the Department of Ophthalmology, Oculoplastics and Orbital Surgery at Emory University School of Medicine. Contact Dr. Murchison at
1. Tucker B. Two cases of dislocation of the eyeball through the palpebral fissure. J Nerv Ment Dis 1907;34:391-7.
2. Kunesh JC, Katz SE. Spontaneous globe luxation associated with contact lens placement. CLAO J 2002;28:2-4.
3. Apostolopoulos M, et al. Bilateral optic neuropathy associated with voluntary globe subluxation and floppy eyelid syndrome. Arch Ophthalmol 2004;122:1555-6.
4. Alexandrakis G, Tse DT, Chang WJ. Spontaneous globe luxation associated with floppy eyelid syndrome and shallow orbits. Arch Ophthalmol 1999;117:138-9.
5. Tse, DT. A simple maneuver to reposit a subluxed globe. Arch Ophthalmol 2000;118:410-411.
6. Wood C, Pearson A, Craft A, et.al. Globe luxation in histiocytosis X. Br J Ophthalmol 1988;72:621-3.
7. Chandran G, Alexander T, Thomas A. Crouzon's disease with bilateral luxation of the globes. Indian J Ophthalmol 1981;28:229-30.