Already shown to be useful for phakic correction, this lens platform has been used worldwide for many years and is now starting to be implanted in
Joshua C. Teichman, MD, and Iqbal Ike K. Ahmed, MD, FRCSC, Toronto
In cases requiring primary or secondary intraocular lens implantation in eyes lacking capsular support, an anterior chamber (AC) IOL, scleral sutured posterior chamber (PC) IOL or an iris-sutured PCIOL are accepted options. These types of patients have either had a history of cataract surgery, typically many years ago, and were left aphakic, or have had IOL complications such as IOL dislocation requiring IOL exchange.
Although it is technically easier to implant an ACIOL, appropriate sizing is a concern, as angle-to-angle dimensions vary considerably between patients, thus leading to inherent risks of corneal decompensation, new-onset or worsening glaucoma, and chronic inflammation.1 Lastly, a large incision of 6 mm is needed to implant current ACIOLs. 
Scleral sutured PCIOLs have the advantage of being both anatomically closer to the original IOL location enjoying a history of good visual results; unfortunately, they are technically challenging to insert, with an increased risk of IOL tilt and scleral needle passes that increase the risk of intraocular hemorrhage, suture breakage and endophthalmitis.2
Iris suturing also positions the IOL near where a capsular IOL would be, without the risks of scleral suture passes. Although less demanding than scleral suturing, iris fixation can be technically challenging through a limbal incision and there is potential for iris-chafing, pigment dispersion and chronic inflammation.1 As with any sutured IOL, suture breakage, or slippage of the haptic through this suture knot is also a concern.
Although not commonly used in
The Artisan Lens
The Artisan lens (Ophtec, 
As opposed to previous iris clip designs that were associated with iritis, cystoid macular edema and dislocation, the Artisan IOL is fixated to the mid-peripheral iris and centered over the pupil (See Figure 2). In this location, it does not affect mydriasis, iris vasculature or damage the delicate structures of the angle. The lenses are a safe distance from the corneal endothelium, particularly in the aphakic eye. Further, there are no sutures required to support the lens; nor is angle anatomy a concern or issue. Although sufficient iris tissue is required for support, suture pupilloplasty may be employed if needed to reform the pupil, and the IOL may be placed in any axis desired.
Although the Artisan platform for aphakia has been available for many years with more than 300,000 lens implanted worldwide—many used for intracapsular cataract extraction in developing countries—it wasn't until the phakic platform, marketed as "Verisyse," became available in North America that the iris-claw IOL design gained attention in the 
Clinical Results
Clinical results for both the aphakic and phakic lens have been reported, with favorable visual results and low intraoperative and postoperative complication rates.
A 10-year study of 89 eyes implanted with the Artisan lens as a phakic IOL was recently published and demonstrated that the lens was a safe and effective method of correcting moderate to high myopia when strict inclusion criteria were applied.4 The study also concluded the complications were rare, and there was no significant corneal endothelial loss associated with the lens. At 10 years, the mean endothelial cell loss was -8.86 ±16.01 percent compared to expected physiologic loss of 0.6 percent per year.
Another study published in 2005 of 16 eyes after 36 months concluded that the Artisan aphakic IOL was a safe and effective option for implantation in eyes without capsular support.5
Our experience with more than 20 Artisan aphakic IOL implantations has been for two distinct indications: primary implantation in cases with poor capsulo-zonular support; and secondary implantation for either aphakia, or for IOL exchange due to IOL complications. Our results reflect what has been reported in the literature, in this somewhat different patient mix in the first known series in
In the first group, we have used the Artisan IOL in cases where endocapsular IOL fixation was not appropriate, even with the use of a (sutured) capsular tension device—particularly an issue with megalocornea patients in whom commonly available PCIOLs are too small for the capsular bag, and ACIOLs too small for the anterior chamber.
In secondary implantation, we have used the Artisan platform for primary aphakia in patients lacking capsular support, as well as an exchange IOL in cases requiring IOL exchange. These patients include late in-the-bag IOL dislocations in pseudoexfoliation syndrome, spontaneous traumatic IOL dislocations, and in uveitis-glaucoma-hyphema (UGH) syndrome.

Surgical Technique Pearls
One of the significant benefits of the Artisan IOL is the simplified surgical technique. Requirements for successful implantation include: removal of vitreous from the anterior chamber; at least 270 degrees of iris tissue with pupil size smaller than 6 mm (suture pupilloplasty may be required to reform pupil to provide this); and an anterior chamber depth of 3 mm or greater. Miochol-E (Novartis Ophthalmics) aids in constricting the pupil.
We employ a pars plana incision if vitrectomy or IOL explanation is required as part of the procedure to improve access. A cohesive viscoelastic is helpful to maintain the anterior chamber, which may need to be replenished during IOL fixation. Alternatively, an AC maintainer may be used. Maintenance of the anterior chamber is critical to ensure safety and prevent vitreous prolapse.
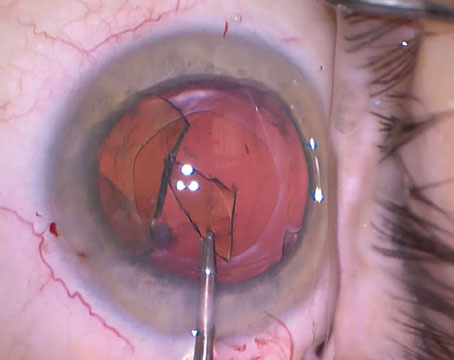
A 5.5-mm incision, which may be made either through a scleral tunnel or corneo-limbal, is required to insert the IOL into the eye with non-toothed forceps. We typically suture this incision with a running 10-0 nylon cross-stitch. Once in the AC, the Artisan lens is rotated to the desired axis, which is typically horizontal, or in the axis of greatest iris support (See Figure 3). It is important to lay the lens in a centered position based on the visual axis of the eye, not necessarily the pupillary axis, although we have found a few millimeter decentration has minimal impact if any on visual results in our patient population.
"Enclavation" of the mid-peripheral iris into the haptics of the lens is probably the most technical part of the procedure. This traditionally has been accomplished using an enclavation needle to sweep the iris up and through the flexible PMMA haptics (See Figure 4). However, as opposed to phakic patients in which the iris is of normal consistency, and readily moves forward due to some positive pressure, the aphakic iris is somewhat different. These irides tend to often be stiff and difficult to grasp with the needle, or may be friable and tear easily due to atrophy.
We have found the use of micro-instrumentation, such as the MST micro anterior segment set (Microsurgical Technologies, mst-surgical.com), including micrograspers and microtying forceps, provides further control and ease in implantation (See Figure 5a, b).
When enclavating iris, two contact points are required: one holding the IOL to provide counter-resistance; and second, lifting the iris into the claw haptics. Further, this should be done with minimal collapse of the anterior chamber. Using micro-instrumentation through small paracentesis incisions helps to maintain a closed system. We prefer using the microtying forceps, rotated 90 degrees to hold the optic while the micrograspers, with their sharper and serrated tips, are used to grasp the iris under the haptics and lift it up into the haptic. This approach seems to enhance and provide a more consistent enclavation (See Figures 6, 7).
The Artisan iris-fixated IOL merges the benefits of ACIOL and sutured PCIOL technology into a simplified and effective implant and technique for correction of aphakia in the absence of capsular support. It has been a very useful implant for primary aphakia, or in cases requiring IOL exchange due to IOL dislocation or complications.
Dr. Teichman is a research fellow at the
1. Condon GP, Masket S, Kranemann C, et al. Small-incision iris fixation of foldable intraocular lenses in the absence of capsule support. Ophthalmology 2007;114:1311-1318.
2. Evereklioglu C, Er H, Bekir NA, et al. Comparison of secondary implantation of flexible open-loop anterior chamber and scleral-fixated posterior chamber intraocular lenses. J Cataract Refract Surg 2003;29:301-308.
3. Worst JG, Massaro RG, Ludwig HH. The introduction of an artificial lens into the eye using Binkhorst's technique. Ophthalmologica 1972;164(5):387-391.
4. Tahzib NG, Nuijts RM,
5. Guell JL, Velasco F, Malecaze F, et al. Secondary Artisan-Verysise aphakic lens implantation. J Cataract Refract Surg 2005;31:2266-2271.