|
| The Tecnis ZKB00 has fewer diffractive rings than other versions, producing a low-add power (+2.75 D) that can be beneficial to patients who want intermediate vision. |
In this article, surgeons discuss the benefits of low- and mid-add multifocal lenses, and why they may be more attractive options for patients than lenses with higher add powers.
High-add Issues
Surgeons say implanting a high-add multifocal, such as a +4 D, would often take a lot of adjustment on the patient’s part.
“With the original, higher-add lenses, I’d routinely counsel patients about the focal point of the add,” recalls Bakersfield, Calif., surgeon Daniel Chang. “Particularly for patients who were younger and still working and/or using the computer a lot, that intermediate computer range was not at the lens’s best focal point. I’d let them know they might have to adjust where their computer screen sat. To look at the computer at the back of their desk, there was a dip in the vision at that distance and it would be blurrier. The high-add lenses had an optimal focal point of about 14 inches, but, functionally, a lot of things in patients’ lives was beyond that, more in the 20-inch range.”
Iselin, N.J., ophthalmologist Doug Grayson says the high-add patients’ visual needs would sometimes confuse even health-care staff. “When we were implanting the [Tecnis] ZMB00, they’d lose the intermediate zone of vision,” he says. “If patients needed computer vision, we were actually giving them -1 D glasses to bring their vision out a little farther. That was the only solution. Some referring optometrists didn’t understand the concept that they were dealing with a multifocal that had almost too-high of an add power. They were giving these patients +1 D reading glasses for the computer, but the concept is that you have to decrease the add for that distance. So, I’d end up calling them and asking them to give the patients a -1 D spectacle.”
New Adds, New Options
Surgeons say the newer add powers in the middle and low range bring a couple of benefits.
• The intermediate focal point. Los Altos, Calif., surgeon Bryan Lee says low- and mid-power adds mesh better with many patients’ activities. “Compared to the stronger-add multifocals, the lower adds give patients a lot more intermediate vision,” he says. “Our world has kind of changed. There are a lot more things today that we use our intermediate vision for than we used to, especially when you consider tablet, desktop and laptop computers, which are even being used more frequently by our cataract-age patients. Patients are willing to trade a little fine print reading ability for better intermediate vision. Also, a low- or mid-add doesn’t just improve their functional vision, it also gives a more continuous range of vision.”
Jeffersonville, Ind., ophthalmologist Asim Piracha says this smoother transition between intermediate and far vision in the low add powers is a result of pushing the focal point out a little farther. “I think of the mid- and low-add multifocal IOLs as kind of progressive lenses vs. the high-adds, which are more like bifocals,” he says. “With the high-add, you get near and you get far, and nothing else. And it’s a really close near, so the intermediate to far-intermediate vision is just gone. This is why the patients with +4 D multifocals will need computer glasses. So the near vision is great, but the overall vision isn’t very functional for many patients with a high-add lens. The low-add patients get intermediate to near vision, and they can see beyond arm’s length, so it’s good for phones, iPads, computers, laptops, the dinner table, car dashboards, and the like. It’s a range of vision, while before, with a high-add, it was more like a bifocal, where you’d have near and then it would just drop off, and then you’d have distance vision.
“The other thing is, there’s more room for error with the low-add lens,” Dr. Piracha adds. “So if a low-add patient is ±0.5 D postop, especially if it’s -0.5 D, he’s pretty happy because he’ll have good distance vision, maybe 20/30, and still have good near. Because of this, I’ve been trying to target about -0.25 D on these low adds, so if I’m off I’ll be off a bit on the minus side, and they’ll still be happy with their distance vision. This is different from the high-add lenses, such as the +4 D, where if the patient isn’t perfectly plano he’s unhappy.”
Dr. Chang says the idea of needing glasses to read some fine print or perform near tasks seems to sit better with patients than having a sudden drop in vision between near and far. “I’ll counsel the low-add patients that they’ll still need glasses for really small print, and the FDA data shows that,” he explains. “For them, it kind of makes sense to need reading glasses occasionally for small print, but to have a drop-off in their vision at the intermediate distance, as is the case with the high-add lenses, doesn’t make as much sense, and is a little bit harder to deal with.”
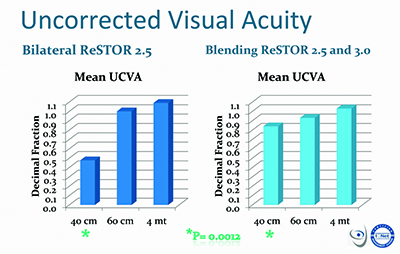 |
| Milan’s Francesco Carones performed a study comparing the results of bilateral implantation of the low-add ReSTOR 2.5 with a blended approach in which one eye gets the 2.5 and the other gets the 3.0. He says that though there may be more night-vision issues with the blended approach, it provides better near vision, as shown in the graph. |
• Diminished halos and night-vision complaints. In some sense, this benefit of the low- and mid-add lenses could be a bigger boon to patients than enhanced intermediate vision, since it makes the lenses more tolerable for the patient and less problematic for surgeons to manage postop.
Surgeons have noticed that patients complain less about night-vision issues, glare and halos with lower-add multifocal lenses, and the data bears this out. In the FDA study of the Tecnis 2.75 D for example, the lens had fewer night-vision complaints than the 3.25-D. Interestingly, it also had fewer night-vision complaints than the Tecnis monofocal control lens: 8.5 percent of 2.75-D patients reported moderate difficulty seeing at night vs. 9.7 percent with the monofocal, and only 0.7 percent reported severe difficulty vs. 4.1 percent with the monofocal IOL.2 Though the ReSTOR 2.5-D trial didn’t look at night-vision problems, the lens did post a slightly lower percentage of moderate and severe glare problems than the 4 D.1,3
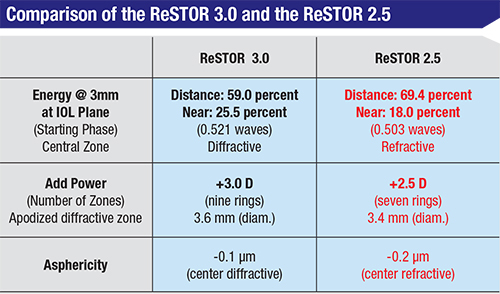
Surgeons say the improvement in visual complaints is a result of both design elements, and the lower power add resulting in a smaller diffractive effect (i.e., fewer diffractive rings on the IOL), which translates into fewer visual complaints. “In the ReSTOR lens in particular, the central element has fewer rings,” explains Bret Fisher, MD, of Panama City, Fla. “And the overall diffractive region of the lens is smaller compared to the 3-D add. There’s also a new central refractive zone, as well as a larger peripheral refractive zone, both used for distance vision. The combination of fewer rings and the presence of these refractive zones really acts to minimize the dysphotopsias patients have at night.”
Dr. Chang says that, on the 2.75-D Tecnis, the halos are simply smaller than on higher-add versions. “Basically, the halo that the patient sees is the energy directed toward the near focal point,” he explains. “So, when you’re looking at a distant point source of light, it’s out of focus and is instead focused on the retina as a halo. So, the higher your add in the lens, the bigger your halo. In other words, the 4-D Tecnis has a certain size halo, the 3.25-D has a smaller halo and the 2.75-D has an even smaller halo. In fact, in the past, when patients with higher-add multifocals in my practice would complain about halos, it almost always was because of the halo’s size rather than its brightness. Specifically, they’d complain that the halo was too large, and that it was blocking their view of cars coming toward them at night. So, the low-add multifocals make these halos smaller. If you look at the night-vision complaint statistics on the Tecnis package insert, the halo complaints get progressively smaller as the add power decreases. There was even less difficulty at night with the low-add multifocal than with the monofocal control in the FDA approval data. That’s surprising. By way of explanation, I think that, for patients, the advantage of having some add power that allows them to see their dashboard at night outweighs the disadvantage that halos produce. In fact, if you look at the halo data as an isolated complaint with the 2.75-D multifocal, it was higher than with the monofocal—but patient satisfaction was higher and night-vision complaints were lower. I think if you look at the big picture, people like the low add.
“I’d prefer to induce fewer night-vision symptoms in patients and have near vision that wasn’t quite as sharp, because you can use reading glasses for the up-close things if you really want to see them,” Dr. Chang continues. “But, you can’t magically make halos and night-vision
complaints go away.”
Patient Selection
Though the low-add multifocals can be useful for many patients, surgeons say you still have to do your due diligence ahead of time to choose the right lens—or maybe even blend two add powers—to get the best results.
Dr. Piracha makes sure to have a thorough conversation with the patient about his occupation and any hobbies. “I have implanted a few Tecnis 3.25-D lenses, but 95 percent are the 2.75 D,” he says. “The ones for whom I recommend the 3.25 are those who say they read all the time, or ‘I want to read in bed,’ or ‘I want to be able to read a book, but I’m not on the computer that much,’ or the patient who says he likes to hold things up close while doing fine needlework or woodworking. These are usually the older patients; the same patients who would have done fine with the 4 D will do even better with the 3.25 D. However, if they mostly use the intermediate distance, such as working on the computer, or if they’re a driver by trade and night vision is important to them, I’ll use the low-add lens. A lot of my patients like to shoot rifles, so what’s nice with the low-add lens is they can see both the target and the gun sight simultaneously. That’s something monovision can’t do. One of my patients owns his own shooting range, competes professionally and trains kids, and he’s thrilled with the low-add lens.” Some surgeons will also give patients questionnaires about their activities in order to select the right lens for them.
Dr. Chang likes to observe how the patient reads firsthand. “I’ll hand him a brochure or some other educational material for him to review and just look at where he holds it,” he says. “I watch where he automatically holds it, whether it’s because of his glasses, his current prescription or whatever. I use that range as a guide for which lens I’m going to start with. So, if he holds the material up close, then I’ll offer him a 3.25 D or potentially even a 4 D. If he holds it farther out, I’ll go for the 2.75-D add.”
 |
Dr. Carones studied the results of this blending approach in 40 patients, comparing the results to 20 patients who received bilateral 2.5-D ReSTORs. Postop, in the bilateral 2.5-D group, all patients were 20/20 uncorrected for distance, and all saw 20/20 or better uncorrected at intermediate (measured as 60 cm in the study). Only six patients (30 percent) had 20/20 at 40 cm, while all saw at least 20/50 at that range. In the blended group, Dr. Carones says you can see an expanded range of vision at near: All could see 20/20 at distance. Ninety-three percent saw 20/20 or better at intermediate, and 70 percent saw 20/20 or better at near, with everyone in the group seeing at least 20/32 at near.
In day-to-day practice, surgeons say this blending can often make sense for patients. “In the first eye, I usually implant the lowest add power,” says Dr. Lee. “I’ll then wait a little longer than usual for the patient to recover since it’s a multifocal. That way, the patient has time to get used to the multifocal. When he comes back for a postop visit, I’ll talk to him about the function of that first eye, asking such questions as, ‘Do you like it? Do you want the second eye to match it? Would you instead appreciate having some more reading-distance vision in the second eye?’ ” If he says he’d prefer more reading vision, I’ll go for the intermediate power for the second eye. For instance, if I’m using the Tecnis, I’d implant the
3.25-D add.”
Dr. Fisher says the low-add multifocals, such as the AcrySof ReSTOR he uses, can also work when paired with a monofocal IOL that the patient had implanted in the fellow eye years previously. “I’ve done several patients who have had a monofocal IOL in one eye now for years,” he says. “I’ve been able to offer them a lower-add multifocal for the other eye, knowing that they wouldn’t feel as if they were compromising on the distance vision compared to their monofocal lens, and that they were also picking up some intermediate vision. I think that highlights what a good ‘utility player’ these lenses are becoming.” REVIEW
Drs. Fisher and Carones are consultants to Alcon. Drs. Chang and Piracha are consultants to Abbott Medical Optics. Drs. Grayson and Lee have no financial interest in any of the products mentioned.
1. http://www.accessdata.fda.gov/cdrh_docs/pdf4/P040020S050b.pdf. Accessed 14 Dec 2015.
2. http://www.accessdata.fda.gov/cdrh_docs/pdf/P980040S049b.pdf. Accessed 9 Dec 2015.
3. http://www.accessdata.fda.gov/cdrh_docs/pdf4/P040020c.pdf. Accessed 14 Dec 2015.