Diagnosis, Workup and Treatment
Based on the clinical history and exam, the differential diagnosis included infectious conditions such as syphilis, tuberculosis, Lyme disease, toxoplasmosis or fungal infections. The differential diagnosis also included inflammatory and neoplastic conditions such as sarcoidosis, persistent placoid maculopathy, lymphoma or metastasis.
An anterior chamber paracentesis and intravitreal injection of foscarnet, ganciclovir and clindamycin were performed in the Wills ER. The aqueous fluid was sent for toxoplasmosis, herpes zoster, herpes simplex and cytomegalovirus PCR, and all were within normal limits. Additional workup included blood cultures, ACE and lysozyme levels, a head CT looking for calcifications, and a chest X-ray, which were all unremarkable. Laboratory investigation for infectious causes included a PPD, RPR/FTA serum analyses and Lyme studies. The RPR titer came back positive.
The patient was diagnosed with acute ocular syphilis. He had a documented allergy to penicillin, and, thus, was admitted to the hospital for co-management with the Infectious Disease and Medicine Services. An inpatient lumbar puncture showed pleocytosis (>10 WBC/mm3) and an elevated protein level of 76 mg/dL. He underwent penicillin desensitization and then received IV penicillin in standard neurosyphilis therapeutic doses. He was also given topical steroid prednisolone eye drops four times a day in both eyes. Marked reduction in his uveitic cellular reaction occurred within one week of treatment initiation. His visual acuity improved to 20/30 in the right eye and was stable at 20/20 in the left.
| ||||||||||||||||||||||||||||
Discussion
Referred to as “The Great Masquerader,” syphilis has many clinical stages and manifestations, which are nicely summarized and outlined in the table taken from Lutchman, Weisbrod, and Schwartz (See Table 1).1 It is most commonly spread during sexual contact, exposure to infected lesions, or via transplacental transmission.2 While the U.S. incidence of syphilis decreased from 1990 to 2000, the rate steadily increased throughout the next decade.
|
The eye can be affected in any stage of the disease, and ocular involvement has a wide range of manifestations including: papulosquamous lid lesions; loss of eyebrows; papillary conjunctivitis; scleroconjunctivitis; interstitial keratitis; granulomatous anterior uveitis; vitritis; vasculitis; neuroretinitis; choroiditis; papillitis; and serous retinal detachment.4-6
While ocular syphilis is classically described under the secondary stage of the disease, during which there is hematologic dissemination of spirochetes, the presence of ocular involvement suggests central nervous system activity. As a result, it is advised that patients with ocular involvement receive a lumbar puncture. The CDC defines “confirmed” cases of neurosyphilis by a positive CSF-VDRL in a patient with known syphilis. Likewise, the CDC deems neurosyphilis probable or “presumptive” in patients with signs and symptoms of the disease and either CSF pleocytosis or elevated CSF protein without a positive CSF-VDRL.7 The lumbar puncture not only aids in diagnosis and quantification of disease activity but also allows for physicians to establish baseline CSF titers against which response to therapy can be measured.4
The treatment regimen for neurosyphilis is 10 to 21 days of IV penicillin (dose 12 to 24 million units).8 While responses to therapy are often rapid in onset, many physicians feel that retreatment is warranted if CSF has failed to normalize after two years.
It is important to consider HIV screening in patients with syphilitic uveitis. A 2005 study noted that ocular symptoms in syphilis led to the discovery of HIV seropositivity in 25 to 50 percent of patients.4 When considering the subset of ocular syphilis cases in patients co-infected with HIV, some studies have shown that HIV patients are subject to higher rates of treatment failure and relapse despite appropriate therapy.9 In addition, some sources advise a neurosyphilis regimen of systemic penicillin in all HIV-positive patients with syphilitic uveitis since the progression to neurosyphilis is high in this subgroup of patients.6,9
Interestingly, this particular case report demonstrated an entity known as acute syphilitic posterior placoid chorioretinitis (ASPPC), one of the more unique manifestations of ocular syphilis originally described by J. Donald Gass, MD, and colleagues in 1990.8,10 ASPPC is characterized by large solitary placoid lesions in the area of the macula that are pale yellow.
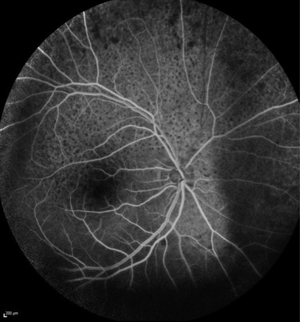
The lesions may have faded centers and coarsely stippled spots of hyperpigmentation.4,8,9,12 Fluorescein angiography of ASPPC shows a distinct pattern of irregular early hypofluorescence with progressive hyperfluorescence overlying persistently less bright foci referred to as “leopard spots”13 (See Figure 3).
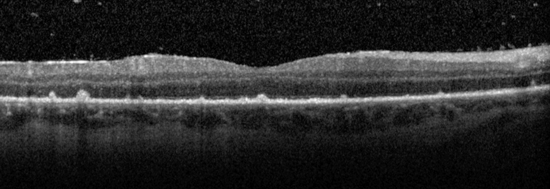
Optical coherence tomography can also be used to demonstrate changes that occur in ASPPC, including disruption of the outer retinal layers (especially within the region of the photoreceptors), loss of the external limiting membrane, hyperreflective and nodular thickening of the retinal pigment epithelium, accumulation of subretinal fluid, loss of normal choroidal vascular detail and diffuse choroidal infiltration8,14,15 (See Figure 4).
|
Optical coherence tomography can also be used to demonstrate changes that occur in ASPPC, including disruption of the outer retinal layers (especially within the region of the photoreceptors), loss of the external limiting membrane, hyperreflective and nodular thickening of the retinal pigment epithelium, accumulation of subretinal fluid, loss of normal choroidal vascular detail and diffuse choroidal infiltration8,14,15 (See Figure 4).
In summary, ASPPC is a distinctive ocular manifestation of syphilis with unique imaging findings. Because risk factors for contracting HIV and syphilis are similar and since co-infection is relatively common, patients diagnosed with syphilis should also be tested for HIV. Penicillin is the treatment of choice for patients with either neurosyphilis or co-infection with HIV. Fortunately, early recognition and appropriate treatment often result in successful control of the disease, but patients with HIV and syphilis should be closely monitored for treatment failure or recurrence.
REVIEW
The author would like to thank
Sonia Mehta, MD, assistant professor, Vitreoretinal Diseases and Surgery, Wills Eye Hospital, for her time and assistance in preparing this case report.
1. Lutchman C, Weisbrod D, Schwartz C. Diagnosis and management of syphilis after unique ocular presentation. Can Fam Physician 2011;57:896-99.
2. Pan S, Yusof N, Hitam W, Noor R, Embong Z. Syphilitic uveitis: Report of 3 cases.” Int J Ophthalmol 2010;3:361-64.
3. Centers for Disease Control and Prevention. 2012 Sexually Transmitted Diseases Surveillance – syphilis. CDC Home. 7 Jan 2014. USA.gov. 29 March 2014.
http://www.cdc.gov/std/stats12/syphilis.htm.
4. Tran T, Cassoux N, Bodaghi B, Fardeau C, Caumes E, Lehoang P. Syphilitic uveitis in patients infected with human immunodeficiency virus. Graefe’s Arch Clin Exp Ophthalmol. 2005;243:863-9. Epub 2005 Mar 15.
5. Tucker J, Li JZ, Robbins GK, Davis BT, et al. Ocular syphilis among HIV-infected patients: A systematic analysis of the literature. Sex Transm Infect. 2011;87:4-8. doi: 10.1136/sti.2010.043042. Epub 2010 Aug 26
6. Nurfahzura M, Hanizasurana H, Zunaina E, Adil H. Successful treatment of syphilitic uveitis in HIV-positive patients. Clin Ophthalmol. 2013;7:1651-4. doi: 10.2147/OPTH.S46876. Epub 2013 Aug 20.
7. Marra, CM. Update on neurosyphilis. Curr Infect Dis Rep 2009;11:127-34.
8. Eandi C, Neri P, Adelman R, Yannuzzi L, Cunningham ET Jr; International Syphilis Study Group. Acute syphilitic posterior placoid chorioretinitis: Report of a case series and comprehensive review of the literature. Retina 2012;32:1915-41.
9. Amaratunge B, Camauglia J, Hall A. Syphilitic uveitis: A review of clinical manifestations and treatment outcomes of syphilitic uveitis in human immunodeficiency virus-positive and negative patients. Clin Experiment Ophthalmol 2010;38:68-74.
10. Gass J, Braunstein R, Chenoweth R. Acute syphilitic posterior placoid chorioretinitis. Ophthalmology 1990;97:1288-97.
11. Yoo C, Kim S, Huh K, Oh J. Atypical acute syphilitic posterior placoid chorioretinitis. Korean J Ophthalmol 2009;23:108-11. doi: 10.3341/kjo.2009.23.2.108. Epub 2009 Jun 9
12. Zamani M, Garfinkel R. Corticosteroid-induced modulation of acute syphilitic posterior placoid chorioretintis. Am J Ophthalmol 2003;135:891-4.
13. Meira-Freitas D, Farah M, Höfling-Lima A, Aggio F. Optical coherence tomography and indocyanine green angiography findings in acute syphilitis posterior placoid choroidopathy: Case report. Arq Bras Oftalmol 2009;72:832-5.
14. Brito P, Penas S, Carneiro A, Palmares J, Reis F. Spectral-domain optical coherence tomography features of acute syphilitic posterior placoid chorioretinitis: The role of autoimmune response in pathogenesis. Case Rep Ophthalmol 2011;2:39-44.
15. Pichi F, Ciardella A, Cunningham ET Jr, Morara M, et al. Spectral domain optical coherence tomography findings in patients with acute syphilitic posterior placod chorioretinopathy. Retina 2013;34:373-84.


