Surgeons need to master the techniques of cataract surgery, but the tools they use also play a part in the success of a procedure, and one of the most important tools at their disposal is the IOL they choose to implant. On this year’s survey of surgeons’ IOL preferences, doctors weigh in on such topics as the attributes of the monofocal lenses they use the most, how their favorite premium IOLs are performing and whether mixing and matching IOLs is a viable strategy.
For this year’s survey, 26 percent of the 10,150 surgeons on the email list opened the survey, and 49 respondents completed it. To learn about their usage patterns, as well as their views on various IOL technologies, read on.
Monocular Options
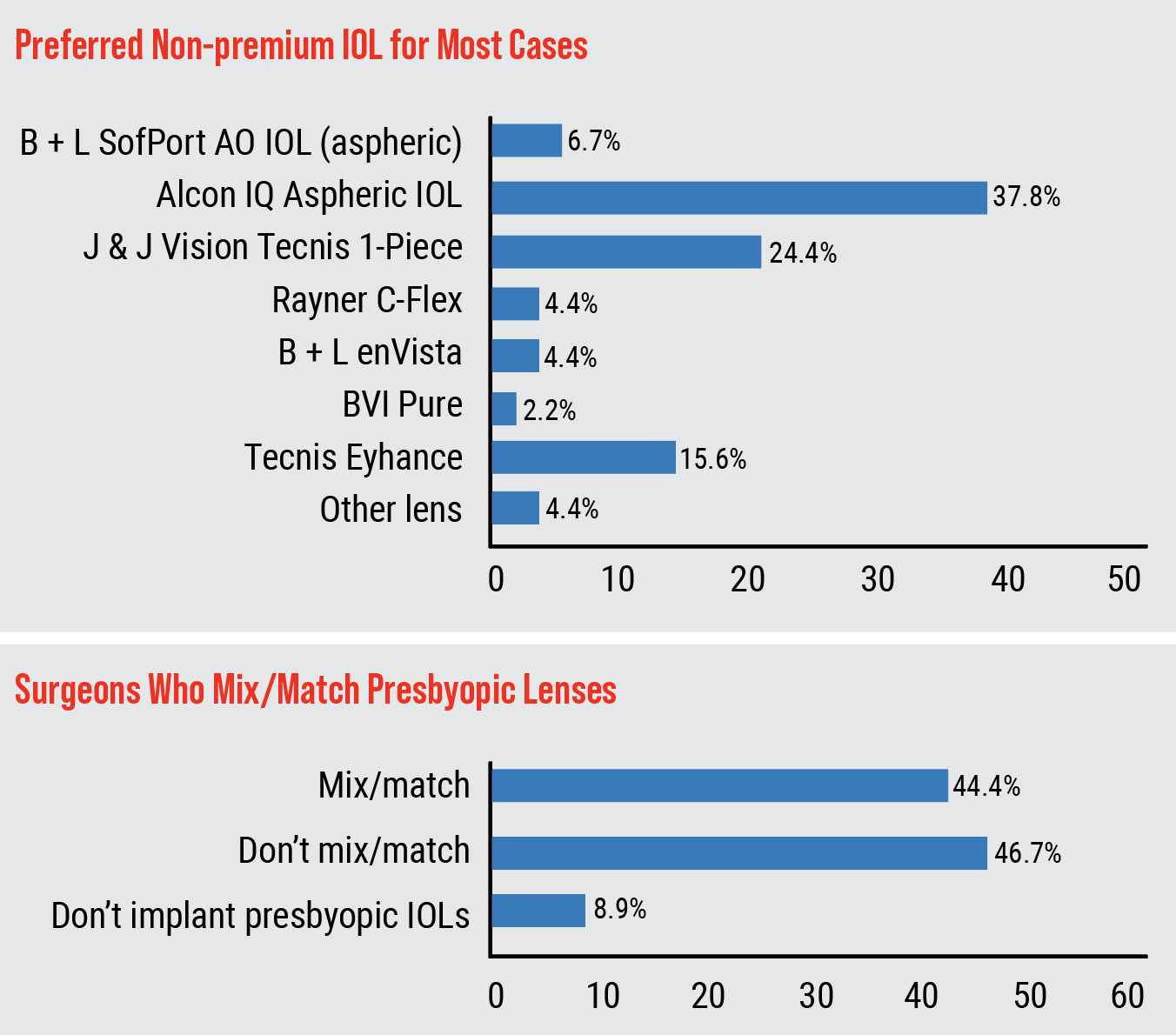
Surgeons opined about their go-to lenses for the bulk of their cases, the monofocal IOLs.
The Alcon IQ Aspheric was the most popular, chosen by 38 percent of the physicians.
Richard Wieder, MD, of St. Louis says he prefers the Alcon IQ because it gives him “long-term great results.” A surgeon from Ohio says he uses the lens because of the “lens material and predictability.” Jonathan Adler, MD, of Bradenton, Florida, likes that the lens has “very few visual obscurations.”
The next most popular lens on the survey was the Johnson & Johnson Tecnis 1-piece, selected by 24 percent of the surgeons. A surgeon from Indiana says she likes the lens for its “superb visual acuity, consistent performance, and outstanding patient outcomes without glistenings.” Louisville, Kentucky, surgeon Asim Piracha uses the lens because it “is clear, has no glistenings, centers well, has a very good preloaded system, has excellent optics, resists scratching, and has negative asphericity.”
The next most popular option was the Tecnis Eyhance (16 percent). “I like the clarity of the lens, the ease of delivery and the fact that it gives some (minimal) EDOF for patients,” says a surgeon from Delaware.
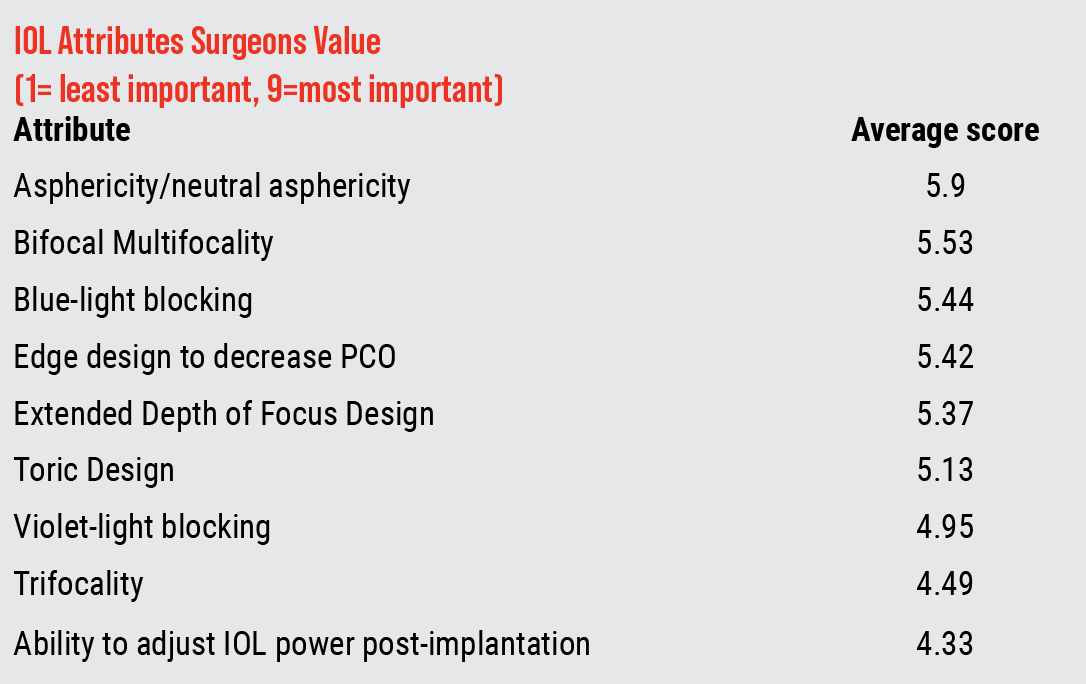
The rest of the surgeons’ choices for non-premium lenses appear in the graph below.
 |
The Premium Arena
Similar to last year’s survey, when it comes to premium lenses, trifocal IOLs were the most popular with the surgeons (some respondents chose more than one option), with the Alcon PanOptix trifocal IOL being used by 35 percent of respondents. However, this is a decrease from last year’s 52 percent, possibly indicating surgeons are giving other options a try. The respondents who implant the PanOptix report that they implant an average of six per month, and charge an average of $3,100 per eye. A Philadelphia surgeon says he gets “good visual results for Clareon Panoptix. I’d like a preloaded option.” A surgeon from North Carolina says he’s satisfied with the lens, but is “still concerned about glistening and I have some concerns about quality of vision and halos.”
The next most popular lens on the survey was the Symfony OptiBlue with InteliLight, chosen by 32.5 percent of surgeons. They say they implant an average of five per month, at an average charge of $1,583/eye.
 |
The Alcon Vivity lens was also chosen by 32.5 percent of the respondents, who average four implants per month at a price of $3,141/eye. “It’s pretty good right now,” says New York City surgeon R. Scott Russell of the Vivity. “Maybe extend the spherical and toric range.” Following the Vivity was the PanOptix toric version, chosen by 30 percent of surgeons, who implant an average of 5.36/month at a price of $2,763.
Richard Wieder, MD, from St. Louis says he likes the “great patient satisfaction” after implanting a PanOptix toric.
The Tecnis Synergy was chosen by 27.5 percent of surgeons. The average number implanted per month on the survey was 3.33, at a price of $3,220/eye. “The lens gives a great range of vision and great contrast sensitivity,” says a Colorado surgeon. I’d love less halos around headlights, but there is no such thing as a free lunch.” Next in line was the toric version of the Symfony OptiBlue/InteliLight, at 25 percent (5.6 implanted/month, $3,020/eye).
The high-tech RxSight Light-adjustable Lens was chosen by 25 percent of the surgeons. The average implanted per month was 15, at a price of $3,658/eye. “It gives excellent, predictable results,” says a Mississippi surgeon. Edward Jones, MD, of Oklahoma City likes the LAL, saying, “No halos. Predictability. Controlled refractive outcome.” A surgeon from New Orleans likes the RxSight, but sees a little room for improvement. “A faster lock adjustment would be nice,” he says. The Alcon Vivity toric also came in at 25 percent (6/month; $2,925/eye).
The Rayner RayOne EMV was selected by 15 percent of the surgeons. The average number implanted per month on the survey was 10, at $1,850/eye). One surgeon likes it for several reasons: “cost, better night-vision profile, and improved near vision without compromising night vision,” he says.
Forty-four percent of the surgeons say they occasionally mix-and-match IOLs (i.e., use different lenses in each eye). There are many possible combinations. A surgeon from Indiana says he mixes “Symfony OptiBlue and synergy. By mixing and matching, I give my patients the benefit of the overall quality of vision and the quality of distance vision of the Symfony OptiBlue, combined with the excellent near vision that the Synergy provides.” A surgeon from California says, “When indicated, I use any combination of Alcon toric: PanOptix and Vivity.” G. Peyton Neatrour, MD, from Virginia Beach, isn’t sold on mixing and matching though. “Mixing increases patient complaints with limited improvement in range of vision,” he says.
 |
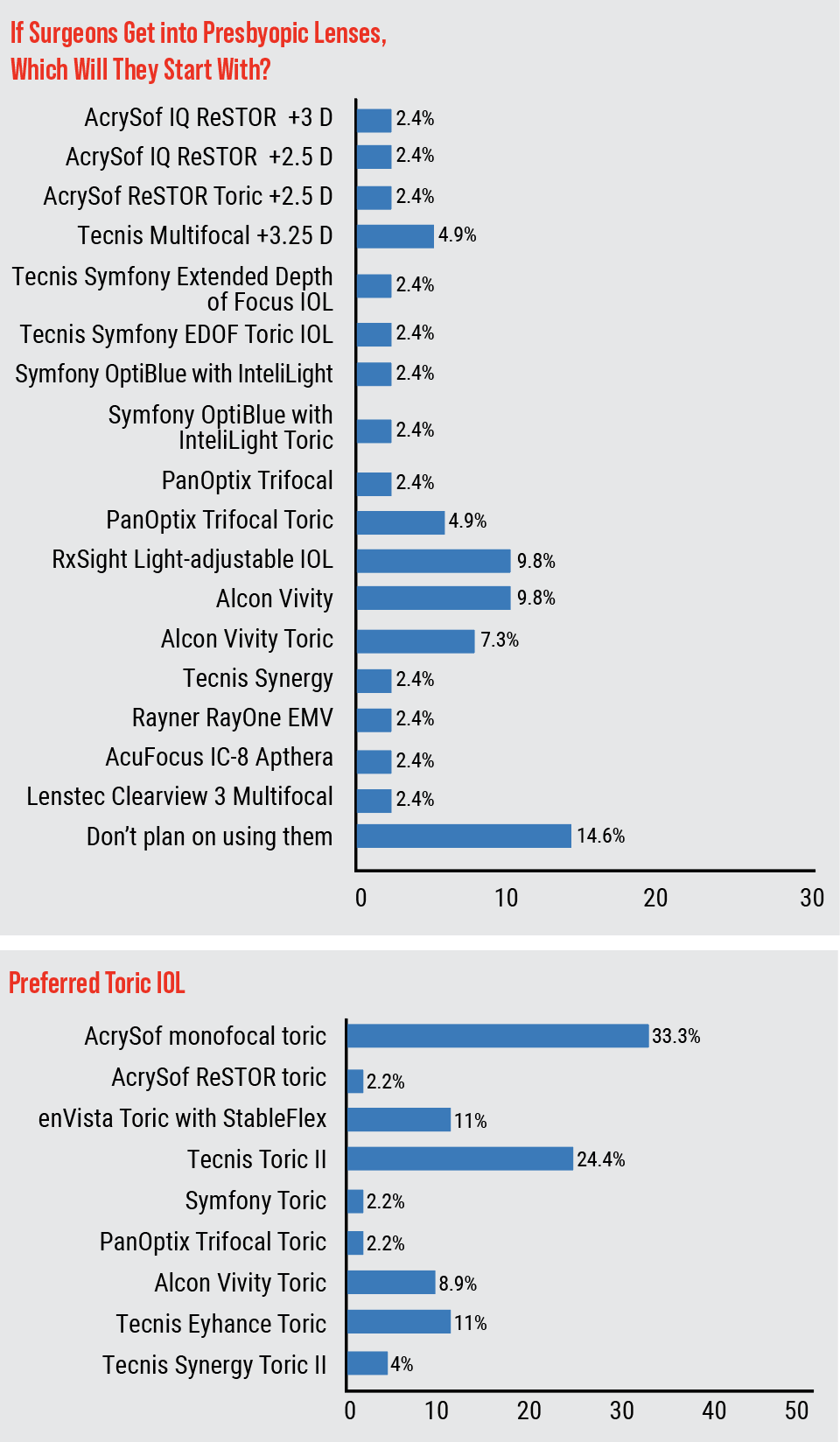
Toric Topics
When it comes to treating patients’ astigmatism, the lens that got the most votes on the survey (33 percent) was the AcrySof monofocal toric. This was followed by the Tecnis Toric II (24 percent) and the enVista Toric with StableFlex (11 percent). The rest of the toric choices appear in the table on pg. 41.
A surgeon from California says he likes the AcrySof toric because of the “stability and wider landing zone.” Krishnarao Rednam, MD, of St. Louis, prefers the Tecnis Toric II because it yields “good visual outcomes.” In the enVista Toric with StableFlex camp is Ronald Glassman, MD, of Teaneck, New Jersey, who says he prefers it because it has “no rotation” and gives “long-term stability.”
 |
The Phakic Option
Twenty-seven percent of the respondents implant phakic IOLs. Their lens of choice is the Staar EVO/EVO+ Visian.
An EVO Visian user from California says, “It’s good for moderate/high myopes if they have enough anatomic space for placement. There are no dry-eye issues, and there’s no increased higher order aberrations.” A surgeon from Philadelphia agrees, saying, “They’re an excellent choice for high myopia.”
The surgeons who don’t implant them have some reservations. John C. Hart Jr., MD, of Farmington Hills, Michigan, says, “I don’t implant these IOLs. Phakic IOLs can be a good option but the cost and risk is greater than corneal refractive surgery.”
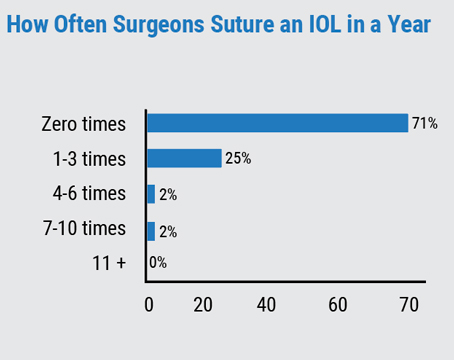
Securing Loose Lenses
Surgeons also opined about situations where a lens needs to be sutured.
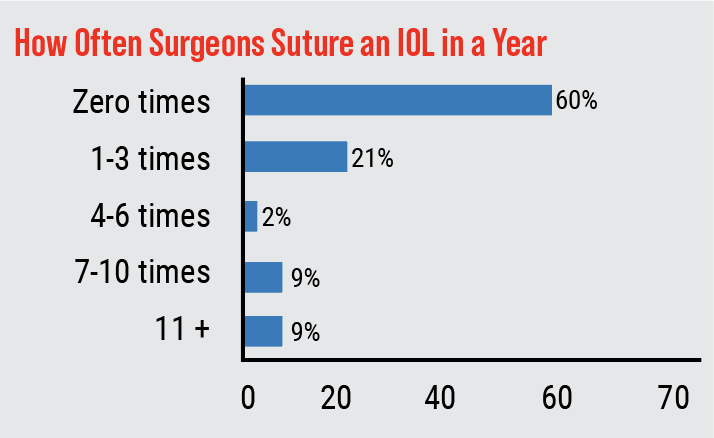
Most of the respondents (60 percent) fortunately don’t have to suture an IOL in any given year. However, 21 percent have to suture one to three lenses, and around 9 percent have to suture 11 or more. The rest of the results appear on the graph to the left.
Some of the reasons cited for suturing include:
- capsular injury;
- dislocated IOL, fixated using a scleral flange technique;
- dislocated lens due to zonule insufficiency, repaired with a scleral suture;
- no capsular support, so the lens is sutured to the iris; and
- a patient who was referred to the surgeon for “dead bag” syndrome.
This article has no commercial sponsorship.