Incision Decisions
Even before they were cleared for cataract surgery, femtosecond lasers were making corneal incisions. Surgeons note, though, that these incisions behave differently from manual ones in certain situations.
“For me, the incisions created by the femtosecond are good,” says Greenville, N.C., surgeon Karl Stonecipher, who works with the Alcon LenSx device. “However, on some patients, such as those with previous RK, there can be a parallax effect that causes the new incisions to not end up where I want them. On these patients, I’ll do these incisions manually because I can see a little bit better that way, and I can get the new incisions placed between the RK incisions. Or, alternately, I can do a scleral tunnel if I feel there are too many RK incisions.”
Harvey Uy, MD, a Lensar system user from Manila, Philippines, says the cornea’s condition may influence the choice of incision. “It’s very important to pay attention to how much corneal arcus or circus senilis is present,” he says. “This grayish-white ring of fatty material, often in the periphery, builds up over the years. Because of the ring’s color, it interferes with the laser treatment in that area and can deflect the laser energy. If you create some portion of your femtosecond incision along a thick band of circus senilis, therefore, the energy will often be deflected and you’ll have an incomplete corneal incision that will be hard to open. In these cases, you can move the incision anterior to the circus location and you’ll be more likely to have a complete incision. In other cases, you may just be better off using a knife for the incision.”
Dilation Issues
|
“There tends to be a pupil constriction reaction when the pupil isn’t too big to begin with,” says Dr. Uy. “Then, when you create your femtosecond capsulorhexis close to the pupil edge, this causes some inflammation that makes the pupil constrict some more. To try to avoid this, preoperatively it helps to add an NSAID to your usual dilation regimen. Also, if you have any control over where to place the capsulorhexis, then you may want to try to put the laser anterior capsulotomy so it’s farther away from the iris, or maybe make the rhexis a little smaller if it helps avoid iris constriction. In rare instances, we’ve had to use some kind of pupil expanding technique.”
Tucson, Ariz., ophthalmologist William Fishkind says that if a surgeon is having a problem with the pupil coming down after the laser, epinephrine in the infusion bottle is one option. “The other is compounded phenylephrine and lidocaine, mixed much like Shugarcaine used to be,” he says. “Introduce 0.2 cc at the beginning of the case. That keeps the pupil dilated throughout the case.”
Hydrodissection
Surgeons say that, in some patients, using hydrodissection in conjunction with the femtosecond laser can be challenging due to the buildup of a gas bubble behind the lens nucleus as a result of the photodisruption. Experts say that simply blasting a fluid wave behind the lens when this gas bubble is present can actually result in a torn posterior capsule.
“There’s a fusion between the cortex and the capsule that locks the fluid in,” explains London, England’s Sheraz Daya, MD, who performs procedures with the Bausch + Lomb Victus laser. “Then, upon the injection of fluid, the capsule breaks. During one case, I was breaking up the lens with a hydrodissection cannula and inadvertently released fluid from the cannula. I noticed it produced a good fluid wave and the lens was mobilized. I then noticed I could deliberately reproduce this in other cases as well, and I use it regularly now. I call the technique translenticular hydrodissection, and Bausch + Lomb has developed a cannula for the maneuver that chops the lens and irrigates at the same time.”
Dr. Fishkind says a surgeon can also hydrodissect in multiple locations. “You have to be careful to hydrodissect in multiple sections because the fluid will sometimes find a plane breaking through the various laser cuts,” he says. “So, for the right eye for example, you inject superiorly, supero-nasally, then directly across from your entry point, then infero-nasally, then inferiorly. Just gently inject the fluid and you’ll find that it separates things better than just going in two places. Injecting in multiple places gets the fluid to separate the cortex from the capsule in more areas, and really helps the I/A at the end of the case, too. The material will be much less adherent.”
Fragmentation and Phaco
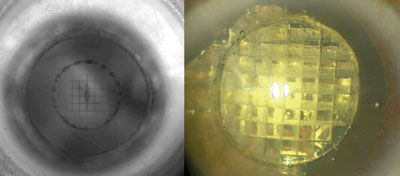
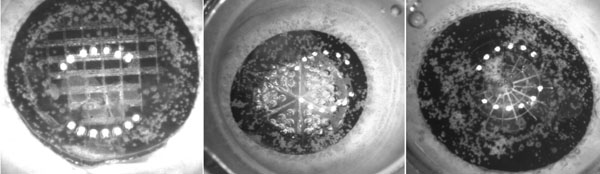
Surgeons say one of the benefits of using a femtosecond laser for cataract surgery is that the laser allows you to soften up the nucleus before you even get into the bag to begin your dividing, flipping or cracking maneuvers. Here are the femto-fragmentation patterns that surgeons say work best, and how to follow them with the best techniques to remove the nuclear material.
|
Dr. Stonecipher uses eight concentric cylinders and six radial chops in what he calls the spider-web pattern. “This is the same technique that Robert Cionni uses,” he explains. “It allows me to bowl out the center into little pixelated pieces and bring in that outer shell. I still can chop, so if I want to chop the lens like in an old-fashioned phaco I can do that. And, in some cases, I’ll do a Brown flip technique and flip the lens right up into the phacoemulsification and it will fall apart into my ultrasound handpiece.
“My approach depends on how the lens presents itself to me,” Dr. Stonecipher continues. “If it’s easily rotated and divides easily, I do divide and conquer. If I get part of it out and the rest isn’t completely broken up, I may do a chop. If it spins easily and flips and collapses in on itself, I’ll use the Brown technique. And, in some of these dense lenses, such as white cataracts and dense brunescent cataracts, I’ll take out the bowl, push into the center and get the epinuclear shell later. In those last cases, I’m trying to protect the endothelium, such as in patients with Fuch’s dystrophy.” Dr. Daya also thinks six segments is ideal. “I just use six segments,” he says. “Four are quite bulky to remove, but if you have too many fragments they can start to fly around and can strike the endothelium.”
Dr. Fishkind says the pre-fragmentation with the laser allows the surgeon to reduce his phaco settings in many cases. “Because the nucleus is softened and pre-chopped, it’s easier to go in with lower power, lower aspiration and lower vacuum,” he says. “It’s kind of easier to get into the center of the nucleus and find one of the pre-established clefts in the pie cuts and crack it as if you’re doing a cracking procedure. Then, once you’ve cracked it into its different pie shapes, you can do a gentle phaco. These segments come out in pieces or chunks; so you lift one up and remove a chunk at the plane of the iris. A vertical chopping technique is not quite as organized as it used to be, because as the segments are lifted up the chunks just come up and then break. You grasp them with aspiration and don’t need very much power to emulsify whatever chunks are coming to you. This is because the chunks are smaller than what you’d get with a normal chopping technique. Also, there are multiples of them because there are a couple of concentric circles, so they fracture into circles as well as pie shapes. The harder the nucleus, the more defined the chunks.”
Using the femtosecond for cataract procedures has led Dr. Rivera to use more venturi-based phaco. “This turns out to be more efficient in removing those smaller cuboidal fragments,” he says. “Besides the instrumentation itself, the fact that I can stay in position two in phaco rather than applying ultrasound position three more aggressively is a huge change. We used to have to apply position three aggressively to ultrasonically emulsify the cataract, but now that’s not the case.”
Dr. Uy says he’s developed an instrument with ASICO for use as the surgeon’s second instrument in his off-hand that helps during phaco. “On one side of the instrument is a nucleus manipulator with a ball-tipped chopper without any sharp edges,” he explains. “I’ve found you don’t really need a sharp edge to break up the cataract because the femtosecond has already broken it up for you. This allows you to manipulate the nuclear fragments better; I’ve found it’s safer to go around the equator to do a sort of horizontal chopping maneuver. The ball tip also allows you to more safely lift up the posterior plate. Since it’s not sharp, there’s no danger of going through the soft cortex and puncturing the posterior capsule. The other side of this combination instrument is like a paddle, which you can use to direct small nuclear fragments to the tip of the phaco handpiece.”
|


“If you have a posterior polar cataract, you generally want to avoid any prechopping,” Dr. Uy continues. “In such a case, we like to do a more routine divide-and-conquer technique. For those cases you can use a pie or a cube pattern with two or three chops, followed by a more gentle divide-and-conquer pattern. If there’s zonular laxity or dialysis, you’ll want to do more fragmentation so that you don’t have to apply as much ultrasound energy to disassemble the nucleus; you won’t have to perform as many maneuvers, just a standard divide and conquer technique. With these cases you also should have hooks ready to support the capsule.
“Finally, a white cataract is one situation where you won’t be able to do much, if any, nuclear fragmentation,” Dr. Uy continues. “The femtosecond is important in these cases, even if you just use it for the capsulorhexis, in order to avoid rupturing the anterior capsule and causing a tear in the posterior capsule that results in the Argentinian-flag sign.”
Dr. Fishkind says an instrument that was on the market 10 or 15 years ago—but which never found a niche—would actually be ideal for femto-phaco. “There used to be a phaco and I/A tip that came in either 0.3- or a 0.5-mm size that never worked for anything,” Dr. Fishkind says. “But now, it would be nice to use in femtosecond cases because you could use the 0.5-mm size to remove the nuclear fragments and then use the 0.3-size for the cortex. With a 0.3-mm I/A tip, for instance, if you grabbed the capsule with it, it wouldn’t tear it. And 0.5-mm I/A tips will take bigger chunks of nucleus and hopefully make things more stable and decrease the risk of tearing the capsule. The other helpful instrument is the rounded Dewey tip. This is a safer phaco tip that’s not very aggressive for traditional phaco. However, it lends itself to laser phaco where you don’t need as much power and you’re removing pieces of material that are already fragmented.”
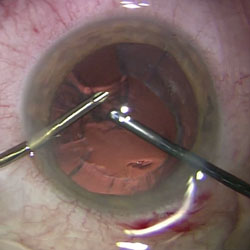
Cortex Challenges
Though some surgeons say they’ve been able to perform femtosecond cataract surgery with minor modifications to their technique, almost all acknowledge that the removal of cortical material is noticeably more challenging than it was with just mechanical and manual phacoemulsification. They’ve developed ways to counteract this difficulty, though.
“The removal of cortical remnants will be one of the biggest learning curves for the surgeon,” says Dr. Stonecipher. “In a manual technique, the cortical pieces are frilly and able to be grabbed easily. In the spots where that femtosecond capsulotomy is performed, however, that capsular-cortical adhesion is tighter. So, if I can’t quite get the cortex to dissect, I’ll start at the posterior capsule and take the cortex up to the back of the anterior capsule as opposed to starting at the top and taking it down. Sometimes, I’ll put the machine on polish mode or low-vacuum mode. That way I’ll work my way backwards if I’m finding it challenging to separate the cortex. I will also tend to use a sideport incision with a bimanual technique. I’ll take the aspiration off and put it on a little instrument, which is just a cannula, and bring it in through the sideport to remove any superior cortex. Also, the sub-incisional cortex can be really hard to get in these cases, so coming in from a different angle helps.”
Dr. Fishkind also says the cortical removal can be confounding, and offers his advice. “There aren’t any tails you can grasp,” he says. “There are no pieces that are sitting out above the capsule that you can grasp and easily maneuver. It’s kind of severed along the capsulorhexis so it’s very smooth. You have to go under the anterior capsule, with the I/A tip pointed up, and with linear vacuum. Go in with zero aspiration and zero vacuum and come up under the anterior capsule, gently increasing either aspiration or vacuum—depending on how you’ve set your machine—with the linear foot pedal until you grasp the cortex and pull it down and centrally to get it away from the anterior capsule. Leave the sub-incisional cortex for last.
“You can usually get the sub-incisional cortex with a sleeved, 45-degree I/A tip from the main incision with maybe a little difficulty,” Dr. Fishkind adds. “But, if you’re stuck you can switch to a bimanual approach to get the sub-incisional cortex.”
Dr. Uy says that, though removing the cortex may be tough, you should try to remain gentle. “There’s a tendency with the femtosecond procedure for cortex to be coagulated and adhere to the anterior capsulorhexis,” he says. “So, you have to be gentle with removing cortex there. It helps if you have a plastic tip or a sleeve instead of metal so you don’t inadvertently cause an enlargement of a capsular tag, and so a nick won’t expand to become a tear.”
Dr. Fishkind says he hopes more work with femtosecond cataract surgery will lead to concrete improvement in results. “My theory about what separates laser cataract surgery from manual surgery isn’t just the wow factor for surgeons,” he says, “rather it’s that it can soften hard nuclei and make them easier to remove so, theoretically, it should be able to remove all nuclei. By doing that—by making this removal easier—it should be safer. And, if femtosecond cataract surgery is safer there would be fewer torn capsules. And if there are fewer torn capsules it would be a wonderful improvement in the safety of cataract surgery.” REVIEW




