With an annual incidence estimated at about 10 to 18 in 100,000 and a prevalence of approximately 0.7%, primary rhegmatogenous retinal detachment represents a treatable cause of otherwise profound, permanent visual loss.1-5 Thus RRD repair represents a core competency of the retinal physician.
Though advances in vitreoretinal surgery have altered trends in choice of repair techniques, the general principles of successful treatment of RRD have remained the same since the popularization of scleral buckling techniques by Charles Schepens and others in the early 1950s.
Specifically, the key principles to successful repair of RRD are identification of rhegmatogenous breaks, relief of traction on causative breaks and treatment of these breaks. These can be accomplished by use of scleral buckling and/or pars-plana vitrectomy. In selected cases, pneumatic retinopexy or demarcation (laser or cryotherapy) may also be considered.
Strengths and Weaknesses
• Scleral buckling. As the standard of care for decades, scleral buckling procedures (SBP) represent a well-understood and reliable method of RRD repair. Advantages offered by SBP include lower incidence of cataract, endophthalmitis, 360-degree support of the vitreous base or peripheral retina, and the ability to perform surgery as an extraocular procedure (except in cases requiring external drainage of subretinal fluid). Additionally, they can be performed in minimally equipped operative settings and for considerably less cost.
Disadvantages include frequent induction of postoperative myopia, difficulty in management of very large and/or posterior retinal breaks and the rare possibilities of buckle erosion or induced strabismus.
 |
A significant disadvantage of vitrectomy in phakic eyes is the development or progression of nuclear sclerotic cataracts. There have also been some suggested long-term associations between vitrectomized, pseudophakic eyes and open-angle glaucoma. There is also some evidence that failed vitrectomy surgery may be associated with more severe proliferative vitreoretinopathy. Additionally, the cost and equipment requirements of vitrectomy are considerably higher than those of pneumatic retinopexy and scleral buckling.
• Pneumatic retinopexy. The key to successful RRD repair with pneumatic retinopexy (PR) is appropriate patient selection. Generally, the ideal patient would have no media opacities to allow full visualization of the retina, single or few breaks located in the upper 6 to 8 eight clock hours of the eye, no larger than 1 clock hour in dimension, and separated by 2 clock hours or less along with a complete posterior vitreous detachment and lack of lattice degeneration.
For those patients felt to be appropriate candidates, the major advantages of this method include the ability to perform it as an office procedure with minimal anesthesia requirement, lower morbidity and post-procedure recovery and significantly lower cost.
| |||||||||||||||||||||||||||||||||||||
 |
| ||||||||||||||||||||||||||||||||||||
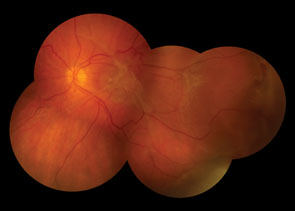
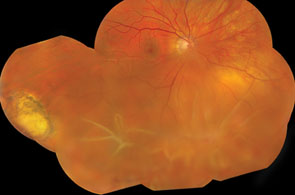
| Figure 2. Proliferative vitreoretinopathy following a scleral buckling procedure. | Figure 3. Proliferative vitreoretinopathy following a vitrectomy. | ||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
Success Rates
Of the repair techniques mentioned, the most broadly applicable are vitrectomy, scleral buckling or a combination of the two. Comparative studies have shown both to be effective, with a trend toward superiority for scleral bucking in phakic patients and toward vitrectomy in pseudphakic patients. Regarding pneumatic retinopexy, studies have indicated a single operation success rate of approximately 80 percent and greater than 95 percent with reoperations.8-11
Trends in Surgical Choice
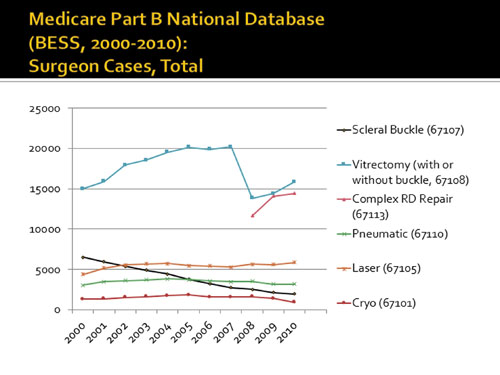
Despite comparable success rates, there has been a clear and well-known trend away from scleral buckling toward primary vitrectomy over the past decade. An analysis of the Medicare fee-for-service database, BESS (Part B Extract Summary System), by CPT code reveals that during the period from 2000 to 2010, scleral buckling fell by two-thirds, while vitrectomy doubled and utilization of other techniques remained stable.
It is likely that factors such as advances in small-gauge vitrectomy surgery, improved wide-angle viewing systems and reduced emphasis on scleral buckling during fellowship training have contributed to these trends.
Failure of Primary RD Repair
• Proliferative vitreoretinopathy. Occurring in 5 to 10 percent of all RRDs and implicated in 75 percent of postoperative redetachments, proliferative vitreoretinopathy is the process involving formation of intravitreal, preretinal or subretinal membranes.19,20 It results from abnormal cellular proliferation at the vitreoretinal interface of fibroblast-like cells, which have been shown to derive from several progenitors, particularly astrocytes and RPE cells.20,21 Early signs include the appearance in the vitreous of pigmented cells and formation of highly cellular membranes. Late changes include an increase in extracellular Type I collagen, in contrast to the Type II collagen of normal vitreous.22
Although rates of postoperative PVR following vitrectomy and SBP have been similar, an important distinction has been the observed phenomenon that when PVR occurs, it is often severe in cases of failed vitrectomy relative to failed SBP. This idea was also supported in a classic experiment in 1984 by Hung-Tao Hsu, MD, and colleagues, in which vitrectomized rabbit eyes developed more severe PVR than nonvitrectomized eyes after intraocular injection of tissue-cultured fibroblasts.23 A recent study of 50 different biomarkers in subretinal fluid from eyes with RRD showed differentially elevated levels of interleukin-3, chemokine ligand-3 and macrophage inhibitory factor, among others.24 Several other studies have implicated a role in overexpression of platelet-derived growth factor.25,26
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
• Other causes. Uncommonly, primary RRD repair may fail unrelated to PVR. In these cases, the failure may result from:
• undiscovered breaks at the time of surgery;• inappropriate choice of surgical technique;• incomplete relief of traction on causative break(s);• incomplete laser/cryotherapy treatment of break(s) or retinotomy; and• inadequate positioning for gas tamponade following surgery.
Managing Failed RRD Repair
Addressing the underlying cause of the retinal redetachment is the standard treatment for failed RRD repair. If previously untreated breaks or new breaks are found to be the cause for redetachment, a return to the operating room is merited, either with repeat vitrectomy, or vitrectomy with scleral buckling.
PVR poses a more difficult challenge, and pharmacologic approaches (steroids, anti-neoplastic/anti-proliferative agents, growth factor pathway inhibitors) that have shown limited success in animal models have not translated into successful management in humans.29-33
When redetachment occurs secondary to PVR, surgical intervention is required and the aims of surgery are to relieve induced tractional forces, to close all retinal breaks and to help maintain ciliary body function. Mild to moderate cases of PVR may be treated with vitrectomy and membrane peeling alone. More severe cases may require the additional support of a scleral buckle as well as membrane peeling, use of perfluorocarbon liquids, relaxing retinotomies and long-term tamponade with silicone oil. REVIEW
Dr. Ahmad is a fellow at The Retina Institute in St. Louis. Dr. Shah is the fellowship director at TRI. Dr. Blinder is an attending surgeon at TRI. The authors have no conflicts of interest or proprietary interests to disclose.
Contact Dr. Ahmad at bahmad@rc-stl.com. Contact Dr. Shah at gkshah1@gmail.com.
1. Wilkes SR, et al., The incidence of retinal detachment in Rochester, Minnesota, 1970-1978. Am J Ophthalmol 1982;94(5):670-3.
2. Coonan P, et al. The incidence of retinal detachment following extracapsular cataract extraction. A ten-year study. Ophthalmology 1985;92:1096-101.
3. Arnold PN. Incidence of retinal detachment. J Cataract Refract Surg 1994 20:363-4.
4. Mitry D, et al. Temporal trends in retinal detachment incidence in Scotland between 1987 and 2006. Br J Ophthalmol 2011;95(3):365-9.
5. Van de Put MA, Hooymans J, Los L. The Incidence of Rhegmatogenous Retinal Detachment in The Netherlands. Ophthalmology 2012 Dec 4. pii: S0161-6420(12)00860-3. doi: 10.1016/j.ophtha.2012.09.001. [Epub ahead of print]
6. Tornambe PE, et al. Pneumatic retinopexy. A two-year follow-up study of the multicenter clinical trial comparing pneumatic retinopexy with scleral buckling. Ophthalmology 1991;98:1115-23.
7. Tornambe PE, Hilton GF. Pneumatic retinopexy. A multicenter randomized controlled clinical trial comparing pneumatic retinopexy with scleral buckling. The Retinal Detachment Study Group. Ophthalmology 1989;96:772-83; discussion 784.
8. Tornambe PE, et al. Expanded indications for pneumatic retinopexy. Ophthalmology;1988 95:597-600.
9. Grizzard WS, et al. Pneumatic retinopexy failures. Cause, prevention, timing, and management. Ophthalmology;1995 102:929-36.
10. Hilton GF, Tornambe PE. Pneumatic retinopexy. An analysis of intraoperative and postoperative complications. The Retinal Detachment Study Group. Retina 1991;11:285-94.
11. Hilton GF, et al. Pneumatic retinopexy. A collaborative report of the first 100 cases. Ophthalmology 1987;94:307-14.
12. Miki D, et al. Comparison of scleral buckling and vitrectomy for retinal detachment resulting from flap tears in superior quadrants. Jpn J Ophthalmol 2001;45(2):187-91.
13. Mansouri A, et al. Recurrent retinal detachment: Does initial treatment matter? Br J Ophthalmol 2010;94:1344-7.
14. Stangos AN, et al., Pars-plana vitrectomy alone vs vitrectomy with scleral buckling for primary rhegmatogenous pseudophakic retinal detachment. Am J Ophthalmol 2004;138:952-8.
15. Sharma YR, et al. Functional and anatomic outcome of scleral buckling versus primary vitrectomy in pseudophakic retinal detachment. Acta Ophthalmol Scand 2005;83:293-7.
16. Brazitikos PD, et al. Primary pars plana vitrectomy versus scleral buckle surgery for the treatment of pseudophakic retinal detachment: a randomized clinical trial. Retina 2005;25:957-64.
17. Weichel ED, et al. Pars plana vitrectomy versus combined pars plana vitrectomy-scleral buckle for primary repair of pseudophakic retinal detachment. Ophthalmology 2006;113:2033-40.
18. Heimann H, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: A prospective randomized multicenter clinical study. Ophthalmology 2007;114:2142-54.
19. No authors listed. The classification of retinal detachment with proliferative vitreoretinopathy. Ophthalmology 1983;90:121-5.
20. Pastor JC. Proliferative vitreoretinopathy: An overview. Surv Ophthalmol 1998;43(1):3-18.
21. Vinores SA, et al. Ultrastructural and immunocytochemical changes in retinal pigment epithelium, retinal glia, and fibroblasts in vitreous culture. Invest Ophthalmol Vis Sci 1990;31:2529-45.
22. Sebag J. The Vitreous: Structure, Function, and Pathobiology. Springer 1989:108-113.
23. Hsu HT, et al. Surgical removal of vitreous. Its effect on intraocular fibroblast proliferation in the rabbit. Arch Ophthalmol 1984;102:605-7.
24. Ricker LJ, et al. Prediction of proliferative vitreoretinopathy after retinal detachment surgery: Potential of biomarker profiling. Am J Ophthalmol 2012;154:347-354 e2.
25. Mori K, et al. Retina-specific expression of PDGF-B versus PDGF-A: Vascular versus nonvascular proliferative retinopathy. Invest Ophthalmol Vis Sci 2002;43:2001-6.
26. Lei H, et al. A potential role for PDGF-C in experimental and clinical proliferative vitreoretinopathy. Invest Ophthalmol Vis Sci 2007;48(5):2335-42.
27. Tewari HK, et al. Comparison of scleral buckling with combined scleral buckling and pars plana vitrectomy in the management of rhegmatogenous retinal detachment with unseen retinal breaks. Clin Experiment Ophthalmol 2003;31(5):403-7.
28. Ahmadieh H, et al. Anatomic and visual outcomes of scleral buckling versus primary vitrectomy in pseudophakic and aphakic retinal detachment: Six-month follow-up results of a single operation--report no. 1. Ophthalmology 2005;112:1421-9.
29. Hui YN, et al. Corticosteroids and daunomycin in the prevention of experimental proliferative vitreoretinopathy induced by macrophages. Graefe’s Arch Clin Exp Ophthalmol 1993;231(2):109-14.
30. Rubsamen PE, Cousins SW. Therapeutic effect of periocular corticosteroids in experimental proliferative vitreoretinopathy. Retina 1997;17:44-50.
31. Wickham L, et al. Randomized controlled trial of combined 5-Fluorouracil and low-molecular-weight heparin in the management of unselected rhegmatogenous retinal detachments undergoing primary vitrectomy. Ophthalmology 2007;114:698-704.
32. Wiedemann P, et al. Adjunctive daunorubicin in the treatment of proliferative vitreoretinopathy: Results of a multicenter clinical trial. Daunomycin Study Group. Am J Ophthalmol 1998;126:550-9.
33. Daniels SA, Coonley K, Yoshizumi M. Taxol treatment of experimental proliferative vitreoretinopathy. Graefe’s Arch Clin Exp Ophthalmol 1990;228(6):513-6.


