You may have heard about Medicare’s new “complexity” code, but haven’t gotten many details on it. In this installment of Medicare Q&A, we’ll answer providers’ common questions about the new code.
Q: What is the new ‘complexity’ code?
HCPCS code +G2211 states: “Visit complexity inherent to evaluation and management associated with medical care services that serve as the continuing focal point for all needed health-care services and/or with medical care services that are part of ongoing care related to a patient’s single, serious condition or a complex condition. (Add-on code, list separately in addition to office/outpatient evaluation and management visit, new or established).”1
Medicare introduced the code in 2021. However, it didn’t go into effect until January 1, 2024. It’s currently covered by CMS. The national, unadjusted allowed amount for HCPCS code +G2211 is $16.04. In terms of third party payors, private payors aren’t required to cover and pay separately for +G2211. Policies vary.
The AMA and most surgical specialty societies opposed implementation of +G2211 due to the required statutory budget neutrality adjustment and resulting 2.18-percent reduction in the 2024 Medicare conversion factor.2,3
Q: When does this code apply?
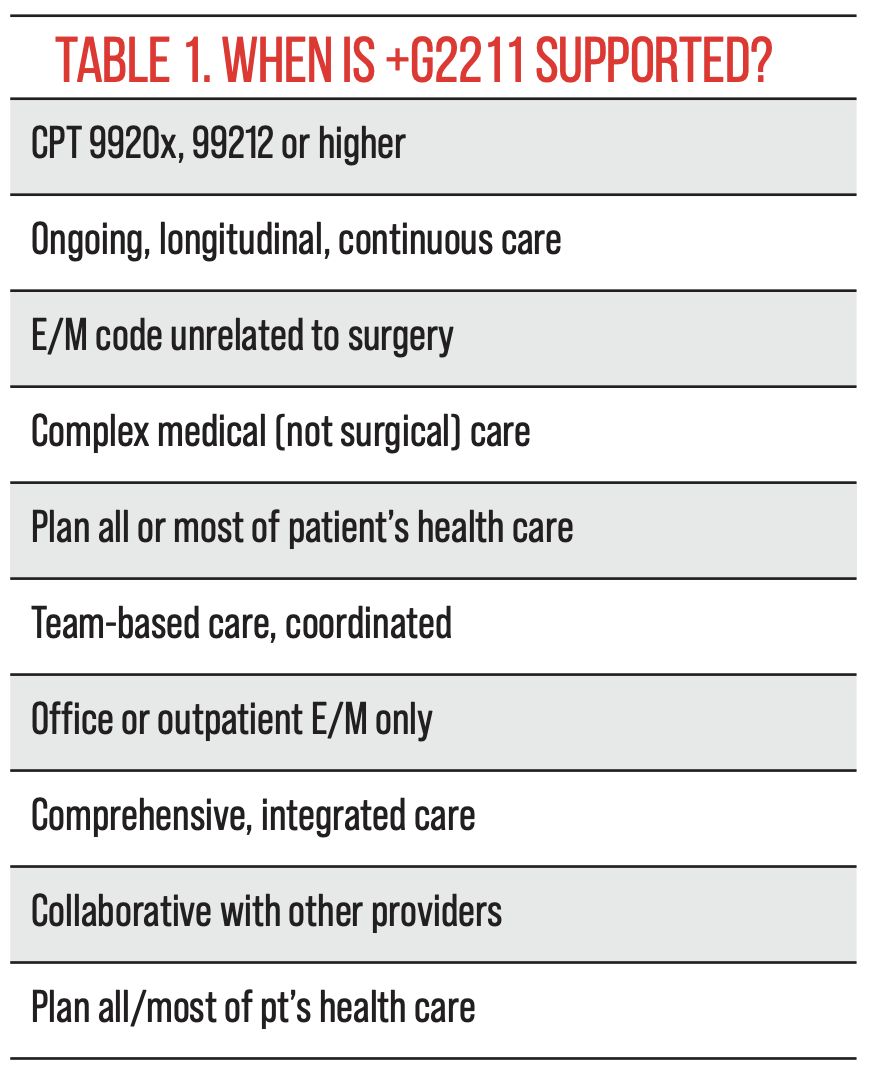
According to the CMS Fact Sheet, “HCPCS code +G2211 includes services that enable practitioners to build longitudinal relationships with all patients (that is, not only those patients who have a chronic condition or single-high risk disease) and to address the majority of patients’ health care needs with consistency and continuity over longer periods of time. This includes furnishing services to patients on an ongoing basis that result in care that is personalized to the patient. The services result in a comprehensive, longitudinal, and continuous relationship with the patient and involve delivery of team-based care that is accessible, coordinated with other practitioners and providers, and integrated with the broader health care landscape….In the context of specialty care, HCPCS code +G2211 could recognize the resources inherent in engaging the patient in a continuous and active collaborative plan of care related to an identified health condition the management of which requires the direction of a clinician with specialized clinical knowledge, skill and experience. Such collaborative care includes patient education, expectations and responsibilities, shared decision-making around therapeutic goals, and shared commitments to achieve those goals.”1
 |
Q: Can ophthalmologists use this code?
While there’s nothing published that precludes ophthalmologists from reporting +G2211 in conjunction with an E/M code, it’s unlikely that this will occur frequently. The code needs to be supported in the medical records by more than simply a long, time consuming encounter.
A particular case example can illustrate how the code may be used:
A neuro-ophthalmologist sees a 41-year-old, Hispanic female for a follow-up visit to review test results. The patient experienced dramatic vision loss three days ago; she experienced a similar episode 13 months prior that resolved with high-dose, oral steroids. At the most recent visit two days ago, the patient complained of headache and difficulty sleeping. A series of tests were ordered: blood tests; MRI; OCT; and VEP. At today’s exam, her vision is light perception in both eyes. A diagnosis of bilateral retrobulbar optic neuritis secondary to multiple sclerosis is made. Based on the Optic Neuritis Treatment Trial,5[4] the neuro-ophthalmologist recommends intravenous steroids.
Immediately after the visit, a discussion occurs between the neuro-ophthalmologist and the patient’s neurologist; interferon therapy is considered. The neurologist admitted the patient to the hospital later that day for IV steroid treatment.5 The neuro-ophthalmologist will reassess the patient in the hospital frequently. The outpatient service of the neuro-ophthalmologist is billed with 99215 and +G2211. The admiszsion of the patient to the hospital by the neurologist is an inpatient service and ineligible to be billed with +G2211.
There’s some similarity to care management services6 in the description of +G2211, particularly where it refers to “plan of care” and “team-based care.” CMS states, “…we do not believe the inherent complexity code would be duplicative of care management services since the inherent complexity better recognizes the professional work within the visit, while the care management codes recognize services that happen outside of the visit.”7
The American Academy of Ophthalmology Fact Sheet cites several examples that don’t support code +G2211:
• exam for ocular trauma, subconjunctival hemorrhage, seasonal allergies, viral conjunctivitis or other conditions that are time-limited in nature;
• exam that results in the decision for surgery to resolve a condition such as cataract or eyelid lesion; and
• exams where comorbidities are not present or not addressed, and/or when the billing practitioner has not taken responsibility for ongoing medical care for that patient with consistency and continuity over time, or does not plan to take responsibility for subsequent, ongoing medical care for that patient with consistency and continuity over time.8
Q: Which E/M services can be reported with +G2211?
HCPCS contains an instruction for +G2211 that says, “Add-on code, list separately in addition to office/outpatient evaluation and management visit, new or established.” It can’t be combined with any other service such as inpatient E/M or eye codes (920xx). Also, it shouldn’t be reported with 99211 or when an E/M service is reported with modifier -25.9,10
Q: What providers can report code +G2211?
All physicians may use +G2211, however CMS says it “…took into account the likelihood that primary care specialties will have a higher utilization of the add-on code than other specialties, surgical specialties will have the lowest utilization since they are less likely to establish longitudinal care relationships with patients, and other specialists are more likely to have longitudinal care relationships than surgical specialties but less likely than primary care specialists.”12 It’s noteworthy that “primary care specialties” doesn’t include ophthalmology or optometry according to CMS.12
Eye care providers’ use of +G2211 should be rare. The characteristics that define this add-on code are not typically applicable in ophthalmology or optometry. The frequent use of it is only expected for primary care specialties. Post-payment audits commonly result from payor perception of inappropriate use.
1. CMS Fact Sheet O/O E/M Visits, January 11, 2021. https://www.cms.gov/files/document/physician-fee-schedule-pfs-payment-officeoutpatient-evaluation-and-management-em-visits-fact-sheet.pdf. Accessed February 16, 2024.
2. CMS Fact Sheet. https://www.cms.gov/newsroom/fact-sheets/calendar-year-cy-2024-medicare-physician-fee-schedule-final-rule. Accessed February 16, 2024.
3. ASCRS. https://ascrs.org/news/washington-watch/ww-november-3-2023. Accessed February 16, 2024.
4. Cleary PA, Beck RW, Anderson MM, Kenny DJ, Backlund J, Gilbert PR, Optic Neuritis Study Group. Design, methods and conduct of the Optic Neuritis Treatment Trial. Control Clin Trials 1993;14:123–42.
5. Menon, V, Saxena, R, Misra, R, Phuljhele, S. Management of optic neuritis. Indian J Ophthalmol 2011;59:2:117-122.
6. American Medical Association. 2024 CPT Professional Edition. Care Management Services.
7. CMS-1784-F. https://www.federalregister.gov/documents/2023/11/16/2023-24184/medicare-and-medicaid-programs-cy-2024-payment-policies-under-the-physician-fee-schedule-and-other. Accessed February 16, 2024
8. AAO. Fact Sheet: Coding for G2211 Visit Complexity Add-on Code. https://www.aao.org/Assets/dc13c710-fb14-4579-9c08-723b53cfca10/638415337512370000/g2211-visit-complexity-pdf?inline=1. Accessed
February 16, 2024.
9. Georgia Academy of Family Physicians. G2211 Add-on Code: What It Is and When To Use It. https://gafp.org/g2211-add-on-code-what-it-is-and-when-to-use-it/#:~:text=Report%20HCPCS%20code%20G2211%20with,is%20reported%20with%20modifier%2025. Accessed February 16, 2024.
10. CMS. MLN Matters. Edits to prevent payment of G2211 with office/outpatient evaluation and management visit and modifier 25. https://www.cms.gov/files/document/mm13272-edits-prevent-payment-g2211-office/outpatient-evaluation-and-management-visit-and-modifier.pdf. Accessed February 16, 2024.
11. CMS-1784-P. Federal Register Aug 7, 2023;88:150:52353. https://www.govinfo.gov/content/pkg/FR-2023-08-07/pdf/2023-16249.pdf. Accessed February 16, 2024.
12. CMS. Evaluation of the primary care first model. https://www.cms.gov/priorities/innovation/data-and-reports/2022/pcf-first-eval-rpt. Accessed February 16, 2024.
Mary Pat Johnson is a senior consultant at the Corcoran Consulting Group and is based in North Carolina. She can be reached at mpjohnson@corcoranccg.com.


