The selection of an academic health center (AHC) chair is the most important choice a health system can make regarding the future of health care in America. Within ophthalmology, this is true whether an ophthalmologist goes into private practice or academics. It’s so important because department chairs recruit and retain clinicians and scientists who train future generations of doctors, discover new cures for disease through research, and deliver high-quality clinical care from these AHC’s across the country.
The ideal chair will possess a combination of traits, such as strategic thinking, communication skills and recruiting prowess, that sets him or her apart from the crowd and allows the health center to excel in its mission. One trait that’s not advertised, however, is that the candidate must have external, peer-reviewed national grant funding (specifically, being a principal investigator [PI] on an R01 National Institutes of Health grant). Is this aspect of a candidate’s curriculum vitae important for departmental chair leadership when weighed against a candidate’s other talents?
This article briefly attempts to explain the process whereby we arrive at these hiring decisions, which traits are important, and what really goes on behind the curtain at most academic health institutions.
Traits for a Successful Chair
As the chair of ophthalmology and the dean of faculty affairs at an academic health center in the Midwest, I have a unique perspective on how AHC’s recruit chairs of departments in all specialties, not just in ophthalmology. The bottom line is that good administrators have many traits in common that most of us would agree are important.
An excellent reference for data on what criteria are preferred when choosing a chair of a medical school department comes from the Association of American Medical Colleges’ series on the structure of the successful medical school department chairs.1 From data garnered from these publications, peer-reviewed literature and personal experience, I believe the following five traits are most important when selecting a chair of ophthalmology, or any other department in a medical school:
- Proven administrative talent
- Recruiting prowess
- Excellent communication skills
- Commitment to the school’s mission
- Strategic thinking ability
- Bonus: PI on an R01 grant
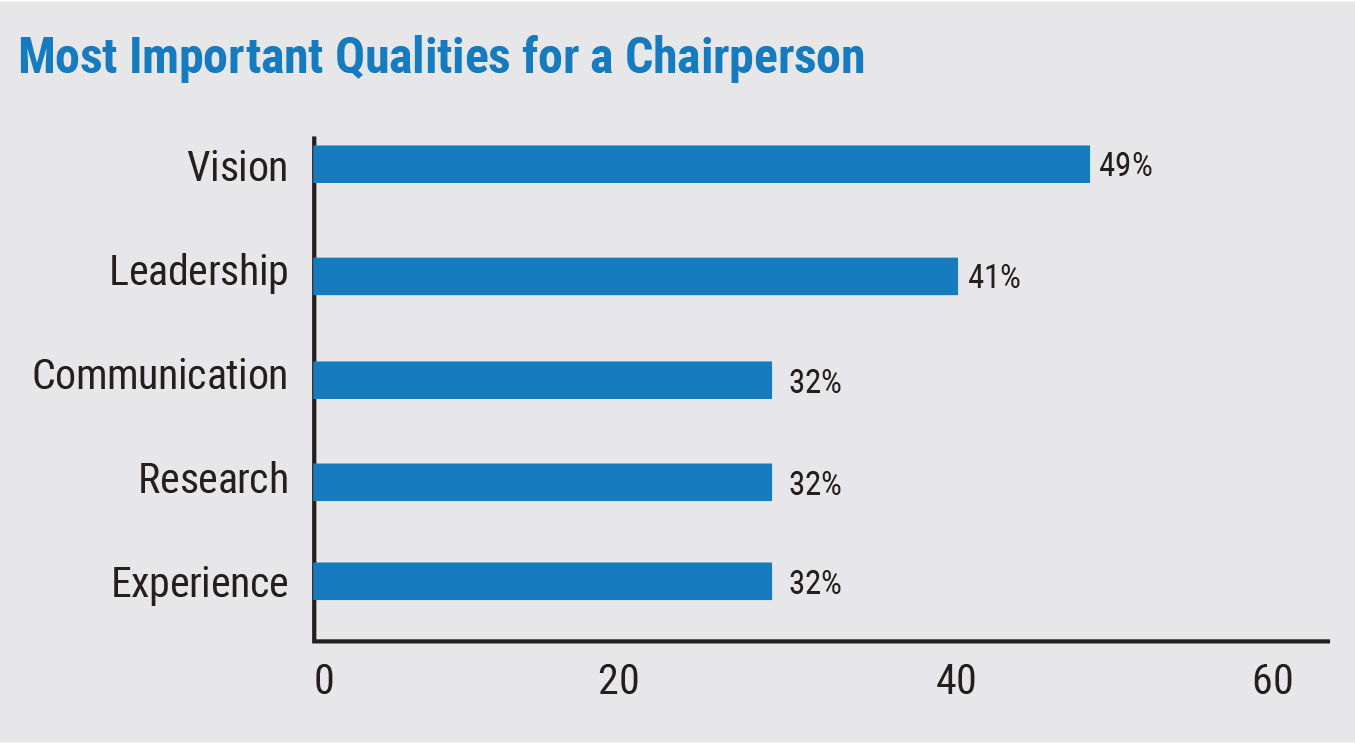
To see whether my colleagues agreed, I sent out an informal survey to all the chairs of departments of ophthalmology from around the country. The following question was asked: “What are considered the top five traits (or qualifications) looked for when filling the position of a chairperson?” Thirty percent (41/134) responded, and the top five answers were vision, leadership, communication, research and experience. A fascinating omission was the requirement that a chairperson have an NIH grant. In fact, from the 41 returned surveys, only two even mentioned a grant. There were 24 total traits suggested by chairs of ophthalmology and number 23 by frequency of answers, was “needs an NIH grant.” A grant was suggested twice in the 41 responses and wasn’t in the top five in any instance.
But what makes the traits enumerated above so important for a chairperson? Each of the preferred chair characteristics mentioned above deserve some explanation:
• Proven administrative talent. Administrative talent is probably learned over time and comes with successes and failures over the course of many years. I tend to think there are very few natural born leaders. Instead, it’s more like a process of iron sharpening iron—the metal is tested over time and gets better. This is often observed in our peers as we become more patient, kind, emotionally in tune with our faculty, and communicate more effectively as we mature into our jobs. It’s a truism that many of us go into the job having very little idea of how to run an academic ophthalmology department, but in the end we either learn and get better or we’re let go. Even so, this trait is of paramount importance in a leader and it’s under-recognized in my experience. Leaders at all levels should create a system whereby they’re looking for this trait. In a way, it encompasses all the other important traits of a departmental chair.
• Recruiting prowess. A chair of a department has two main jobs: set the strategy and vision for the department and recruit well. This latter trait can’t be overstated. If chairs are the lifeblood of medical school leadership, then the faculty they recruit are the lifeblood of the entire school. Research, teaching and clinical care flow from these recruits and a chairperson has to make this a top priority. If a chair isn’t good at recruiting, they need to get good at it. They should talk to their peers, go to training courses, engage with the AAMC and recognize it as vital to both their and the school’s success. There’s no excuse to not recruit effectively if you’re a chair. (For an in-depth discussion on recruiting faculty, see “Confessions of a New Chairman on Recruiting” in Review’s April 2016 issue.)
• Excellent communicator. This is an obvious trait for a leader at any level. What’s important to point out here is that good communicators are good with a variety of audiences. A good chair is good one-on-one, one-on-five and one-on-100. They know their audience and never talk down to them. They’re upbeat, encouraging, positive and moving forward almost always. When faced with challenges, they’re able to convey empathy, compassion, a we-will-fix-this attitude and they’ll talk to all stakeholders involved.
One key to communication is repetition. You don’t just send out an email; you send out an email, talk to the group, talk to each individual and then send out the email again. It’s like wearing a belt with suspenders—but you make sure your pants are also tight.
Communication skills are encompassed in the first trait, being an administrative talent. This skilled is honed over time and is cultivated over many years of trial and error.
 |
|
The most popular answers chosen from a sample of 41 chairs of ophthalmology from around the country. The percentage is the proportion of the respondents who identified that quality as being in the top five most important traits. |
• Commitment to the school’s mission. This concept may sound obvious, but I don’t think it is. Many of us can recite our mission statement from memory, or can at least look it up quickly. The concept here is that it’s more than just teaching, research and service. The idea is that the leader is committed to something greater than themselves: Did they join the Navy to see the world or did they join the Navy so the world could see them, so to speak? Individuals who adopt the values of their institution are easy to trust, follow and understand. In other words, are they loyal to the mission of the school or are they loyal to a variety of other options (possibly even loyal only to themselves)? Commitment to the mission of the medical school is vital in choosing a department chair.
• Strategic thinker. This final trait encompasses many qualities that are important in a chair. If you’re a strategic thinker, you’ll develop emotional intelligence, build an inclusive and diverse department, shore up your weaknesses, learn the financials you aren’t familiar with and address in a logical way the challenges that so many of us face at an AHC. This type of leader has a high IQ and will learn what’s necessary to become successful and remain so. Seeing the forest for the trees while also understanding the tree itself is a good way to think about this kind of leader. So many times, our chairs don’t see the problems, or remain aloof from them. It’s possible they simply don’t understand the problem. Setting strategy and vision is “job one” of a department chair.
All ophthalmologists trained in the United States have experience with the chair of the department during their training. We learned our clinical and surgical skills under the tutelage of our faculty mentors, who were recruited by our chair. We subsequently go out into the world and open our own practices, join a practice or join a university of our own choosing. How a department chair is chosen is important to all of us regardless of the nature of our ophthalmology practice, now or in the future. Our future colleagues will be shaped by these decisions at our medical schools.

|
The Determination Process
Now that you’ve got a sense of the traits of a successful chair, it’s time to discuss how universities evaluate these traits and choose a chairperson.
The selection process is similar at most universities: The dean of the medical school identifies the need, a job posting is distributed nationally, a diverse search committee composed of leaders and stakeholders from within the university is formed, a “dean’s charge” (more on this later) is performed, applicants are screened by the committee, multiple rounds of interviews take place, negotiations ensue and, finally, a new chair is announced. Though this sounds relatively straightforward, there are aspects of the process that aren’t readily evident.
First, the university’s president/chancellor, or similar leader, has a lot to say about the candidate. They convey this strategy to the dean of the medical school. Though the vision and strategy of our leaders is important, university presidents are rarely physicians, and many times aren’t familiar with the culture of medical schools. Because of this, the relationship between a medical school and the university it functions within can be described with one word: misalignment. While it’s acknowledged that there are many different types of governance models at AHC’s, and some medical schools operate independent of the university management, misalignment is a common theme between institutional leaders of universities nationwide and an unfortunate reality within almost all AHC’s. To quote the father of all management gurus, Peter Drucker, “AHC’s are the most complex management organizations.”2 (He didn’t mean this as a compliment.)
At some point during the search for a new chair, the dean will meet with the search committee and convey what he feels is most important when choosing a new department chair in a process called the “dean’s charge.” The charge consists of factors he considers important, which may include some of the traits described above, as well as other ones. The dean is in constant communication with the many layers of governance at the university, including presidents, chancellors, vice chancellors, provosts and other leaders, and brings this perspective to the search committee in the form of a “charge”—as in “Go forth and don’t mess this up.”
Also, in the process of making his charge, the dean emphasizes confidentiality, indicates who makes the decision on hiring (presumably the dean or a designee), and that the search committee is advisory in nature. One would hope that the dean would say what is almost always implied: “This institution will only consider candidates for the chair of the department of ophthalmology if they are a PI on an R01 NIH grant that they can bring with them to our medical school.” Having been a part of multiple search committees at more than one institution, I can tell the reader with assurance, this charge is almost never uttered. The irony here is that, despite all the important traits we’ve already discussed, the presence of an NIH grant is, in many cases, the most important issue for the president or chancellor of the University. In stand-alone medical schools, it may even be the number one priority of the dean. Why is that?
NIH grants, and other types of external peer-review grants (e.g., Department of Defense grants), can lead to tremendous discoveries in the treatment of disease. We’re lucky that our country values research and supports researchers in this way, and this is what sets AHCs apart from other types of health-care organizations. NIH grants bring not only financial support to the university’s research mission, but also tremendous recognition and prestige to the school. A chair of a department in a medical school will probably better understand their PhDs and their MDs who are clinician scientists if the chair has experience with this type of funding for research. NIH grant numbers at a university are also a quantitative way university presidents can compare themselves to each other. A leader is allowed “in the club” so to speak if their school is particularly prodigious in this area.
However, looking at the numbers, an over-emphasis on grant funding may be short-sighted. According to published data, there are 2,824 academic ophthalmologists at U.S. medical schools.3 Only 175 clinician scientists receive federal funding in ophthalmology.4 This means if leaders are choosing a chair of an ophthalmology department who must be a PI on an R01 NIH grant, the pool consists of only 6 percent of all academic ophthalmologists. Unfortunately, this is a very small subset of talent and will exclude many of the top five traits described earlier in the article.
Furthermore, only about 4 percent of clinician scientists who had R01s appeared to have maintained continuous funding, with half of them having not received additional R01 funding 10 years after receiving their first R01.5 Is this because so many of these clinician scientists become department chairs and no longer have time for research? It leads to the question: Is this model of choosing chairs as R01 grant-holding individuals a good strategy if half are not going to receive funding in the future and very few maintain continuous funding throughout their careers? Are university presidents chasing fool’s gold? Once a clinician scientist takes the mantle of administrating the complexities of a large ophthalmology department, is there still time for their research? It’s difficult to know the answers to these questions. Suffice it to say, some individuals seem to be able to “do it all” and the world is a better place because of their abilities. Still, from the data, it’s clear not everyone can do that. If they did, there would not be this huge drop off in research productivity after a clinician scientist becomes a chair of an ophthalmology department.
Unfortunately, if one is an administrative talent but isn’t a PI on an R01 NIH grant, they may not be considered for leadership as a chair of a department. The data on the prevalence of NIH grant-holding chairs can be gathered from the NIH website (https://report.nih.gov/). There are 131 ophthalmology department chairs in the United States and 50 have had, or used to be a PI on, an R01 NIH grant within the past five years (38 percent). Only 24 (18 percent) currently are the PI on an R01 NIH grant.
From this, it appears that close to 40 percent of chairs have, or have had, grant funding and are the PI on an R01 NIH grant. Clearly, there are a number of very good chairs who don’t have grants and a number of very good chairs who do. The point I’m trying to make is that using just one trait as a litmus test for choosing a department chair is unwise. It’s up to us as health-care leaders, faculty, scientists and/or clinicians in private practice who are alumni of an AHC to communicate this to our presidents, provosts, chancellors and other stakeholders in order to avoid that aforementioned institutional misalignment.
Ophthalmology chairs should have proven administrative talent, recruiting prowess, excellent communication skills, a commitment to the mission of our schools and be strategic thinkers. This is who we want to help lead our profession and who we want working alongside us as ophthalmologists, regardless of whether we choose academics or private practice after graduation from our residency program. It’s incumbent on us as ophthalmologists to convey the importance of these traits to our leaders. A PI of an R01 NIH grant is the cherry on top, but not the sundae. Our failure to communicate about this could lead to misalignment.
An administratively talented chair has the ability to create a vision and strategy, build teams around this vision, and then facilitate the process of growth in the missions of excellent clinical care, research and teaching. They do this by effectively recruiting and retaining talented faculty. If the chair has these traits, they know their own strengths and weaknesses. For instance, if the chair isn’t strong in research, but is administratively talented, they’d recognize this and appoint a competent research director.
It’s my hope that the future of health care in America is populated by chairs who minimize misalignment by possessing such leadership traits, with grant funding being a nice, but not necessary, bonus.
Dr. Fraunfelder is the associate dean of Faculty Affairs, and the Chair and Roy E. Mason and Elizabeth Patee Mason Distinguished Professor of Ophthalmology at the University of Missouri.
1. Grigsby RK, Mallon WT. Recruiting: Proven search and hiring practices for the best talent. 3rd ed. Association of American Medical Colleges, 2017.
2. Drucker PF. The Effective executive: The definitive guide to getting the right things done. Collins Business, 1967.
3. Thiessen CR, Venable GT, Ridenhour NC, Kerr NC. Publication productivity for academic ophthalmologists and academic ophthalmology departments in the United States: An analystic report. J Clin Acad Ophthalmol 2016;8:e19-e29.
4. Van Gelder RN. The clinician-scientist in vision science: A rare and endangered species. Transl Vis Sci Technol 2020;9:12:33.
5. Liu EA, Wang SY, Rao RC. Sustaining independent careers in vision research: Demographics and success in second R01 attainment among clinician-scientists from 1985 to 2019. Trans Vis Sci Tech 2020;9:12:32.


