THE WORLD OF COMPUTER PROgramming gave us a great acronym, GIGO--garbage in, garbage out--to describe why computer programs sometimes fail to provide the results their programmers intended. As it turns out, GIGO has applications in many other fields, including wavefront sensing. Occasionally, a patient"s wavefront output doesn"t look right, or, more often, his wavefront refraction doesn"t jibe with his manifest, and the ophthalmologist is left to decide whether or not a clean image went into the device in the first place, or if the manifest deserves more weight than the wavefront refraction. In this article, surgeons share their strategies for handling situations where some aspect of the wavefront doesn"t seem quite right.
Getting a Sharp Wavefront
Greensboro, N.C., surgeon Karl Stonecipher recommends making sure the wavefront image is valid before moving on to calculating a possible refractive target. Here, he uses the WaveLight Allegretto machine he"s currently studying for an FDA trial to explain the steps he takes.
"First, once the wavefront has been taken, we look at the iris image to make sure the display is centered along the pupil margin," he says. "Second, we look to make sure that the eyelid isn"t in the way, and there"s not a dry spot on the cornea. We want to make sure that we"ve got a good image, even before the machine has read it, and also to make sure that the image is the proper 7 mm in diameter."
Next, he moves onto an analyzer screen where he can look at the actual pattern of dots that comprise the wavefront. "We look at the red central dots, the green ones in the mid-periphery, and the blue ones in the outermost area to make sure there"s a good pattern," he explains. "They"ll be either solid, hollow, crowded or just not there. Hollow spots tell you that there"s some information there but not enough to glean the data you need to treat. Absent spots are usually related to something like a dry spot on the cornea, a cataractous change or something in the vitreous. "You may still get a wavefront refraction from the exam," says Dr. Stonecipher, "but if the dot pattern"s bad, it"s noise, not valid data. I had a patient just the other day who had a posterior vitreous detachment and so many vitreous opacities that we couldn"t get a good dot pattern. So, since we couldn"t get a good wavefront, we did a conventional LASIK procedure on him."
|
|
|
Louis Probst, MD |
|
Vitreous changes, lens clouding or corneal opacities such as that shown here can result in bad data on the wavefront map, and the need to switch to a non-custom LASIK. |
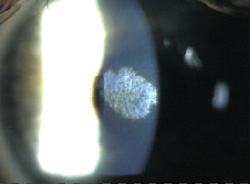
Louis Probst, MD, who practices in Chicago and Madison, Wis., is also mindful of issues that might skew a wavefront refraction. "It can be an opacity on the cornea, an irregular pupil, a pupillary membrane, a very small pupil, or any opacity in the visual system," he says. "In these cases, we"d just perform a conventional treatment because of how the wavefront works, it would be incorrect if it were being blocked or altered in any way." He advises Visx users to be suspicious of wavefront refractions gleaned from pupils that are smaller than 6 mm. "Especially when they get to 5.5 or 5 mm, the results of the wavefront scan don"t seem to be as accurate," he says.
Manifest vs. Wavefront Refractions
In addition to obvious problems with a wavefront capture that will appear on the wavefront image itself, there is also the occasional issue that crops up when the aberrometer"s refraction doesn"t match the manifest refraction.
- Spherical aberration and accommodation. "The most common reason the manifest and wavefront refractions don"t match up is accommodative," says Minneapolis surgeon David Hardten, speaking from his use of the Visx WaveScan system. "So, they"re accommodating on the manifest or on the wavefront."
Accommodation isn"t the only reason for a discrepancy, however.
"If the manifest and wavefront refractions don"t match up, I go back and compare my manifest refraction to a cycloplegic refraction. If those are very similar, then on the wavefront refraction there are two possibilities: The patient could be more myopic on it or more hyperopic on it."
If the patient is more hyperopic on the wavefront refraction, Dr. Hardten says the first possibility to explore is whether the discrepancy could be the result of spherical aberration. To determine if this is the case, compare the wavefront refractions at different pupil sizes that the software allows on the wavefront analyzer. If they change as you change the pupil size, it"s probably spherical aberration, says Dr. Hardten.
As an example, Dr. Hardten offers a hypothetical case of someone who has had LASIK surgery previously, and whose cornea is very flat in the middle but steeper in the mid-periphery. The patient may have a wavefront refraction at a 4-mm pupil size that"s less myopic than the manifest refraction because, with the latter, the patient is being refracted at a 5 or 6 mm pupil. So, at the 3-mm pupil size, the refraction might be plano, at 4 mm it might be -0.75 D, at 5 mm it might be -1.25 D and at 6 mm it might be -1.5 D.
"With this type of patient, as long as you feel comfortable that he isn"t accommodating on the wavefront because you determine that at least one of those refractions is similar to the manifest refraction, then I think that"s a situation where you trust the machine and proceed with the case," explains Dr. Hardten. "What the machine is going to do is correct for the spherical aberration component of it and, hopefully, reduce the variance of the refractive error between the different methods."
Dr. Hardten says that the other reason someone may refract as more hyperopic on the wavefront is a "pretty rare one," but was discussed at a 2004 meeting by London surgeon Julian Stevens. "In some very young patients with an extremely shiny retinal nerve fiber layer, sometimes the wavefront will reflect off of a retinal area that"s more superficial," Dr. Hardten says. "So, the patient may have a more hyperopic refraction by 0.5 D or so. I haven"t seen this personally, but since it was something Dr. Stevens described, I"m on the lookout for it."
If the patient is more myopic on the wavefront refraction than on his manifest, surgeons say this is where accommodation issues appear.
"When you have a patient, usually someone who"s younger, who tends to accommodate during the wavefront test, the wavefront will tend to measure a much more minus prescription than he actually has, and more myopic than the manifest refraction," says Dr. Probst.
David Hardten, MD
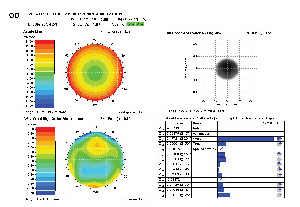
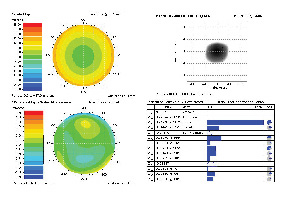
Surgeons say in many cases accommodation can cause the wavefront refraction to appear more myopic than the manifest
refraction. Here, the patient was accommodating at first (top). After relaxing his accommodation, a new refraction was done (bottom).


