Presentation
A 16-year-old woman noted swelling of her right eye for one week. She denied pain or visual acuity changes. She complained of an unrelenting headache for which she was taking Motrin.
Medical History
Past medical history revealed sinusitis and seasonal allergies. She was taking Visine PRN and Claritin PRN. She denied constitutional symptoms.
Examination
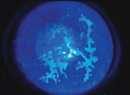
On examination the visual acuity was 20/25, pinhole to 20/20 in the right eye and 20/20 in the left eye. Her pupils were round, equal, briskly reactive and without a relative afferent pupillary defect. Extraocular motility and confrontational visual fields were full in both eyes. Intraocular pressures were 25 mmHg OD and 18 mmHg OS. External examination of the right eye revealed proptosis on the right with an exophthalmometry reading of 24 mm OD and 18 mm OS at a base of 102 mm. In addition she was noted to have inferonasal chemosis with a brownish central discoloration (See Figure 1). The remaining slit lamp and fundus examinations were unremarkable OU, without superficial punctate keratopathy or optic nerve edema. An MRI scan of the orbits was obtained at this time (See Figure 2).
Diagnosis, Workup and Treatment
The presentation of painless proptosis in a teenager can represent infectious, inflammatory or neoplastic processes. Orbital cellulitis, especially in the setting of a history of sinusitis and headaches, must be ruled out. Other considerations include thyroid ophthalmopathy, idiopathic orbital inflammation and eosinophilic granuloma, as well as rhabdomyosarcoma, leukemia and lymphangioma. Imaging must be obtained to further delineate the proptosis. In children, MRI is recommended first line to avoid radiation and to examine soft tissue. CT scan can be quicker to obtain, but there is a small risk related to the radiation exposure.
The patient's clinical presentation and imaging was thought to be consistent with orbital lymphangioma. She was initially observed but returned one week later with increased proptosis, pain and decreased vision (pinhole to 20/60 OD). She was started on prednisone 20 mg twice daily as well as erythromycin ointment and artificial tears to prevent exposure keratopathy. Her proptosis progressed, resulting in severe exposure keratopathy progressing to an inferior corneal ulcer (See Figure 3).
Another MRI was obtained at this time which demonstrated progression of the lesion (See Figure 4). The ulcer was treated with topical antibiotics. Urgent surgical debulking of her orbital lesion was performed, with partial removal of the lesion. Despite decreased proptosis, the patient progressed to have an inferior corneal perforation that was repaired with a corneal patch graft. She was then referred to the Wills Eye Institute Oncology Service. 
On presentation at the Wills Eye Institute, the patient had LP vision OD with 14 mm of proptosis and an intraocular pressure of approximately 30 mmHg. Dilated fundus exam OD showed choroidal folds and dilated tortuous retinal vessels, raising suspicion for an impending vein occlusion. The patient was taken for urgent and complete tumor debulking. Tissue was sent to pathology which revealed a benign vascular lesion with features of lymphangioma and varix, with secondary scarring, hemorrhage, and chronic inflammation. Five weeks postop, her vision was 20/150 and she had no proptosis (See Figure 5).
Discussion
Orbital lymphangioma is a controversial entity for two reasons. First, evidence suggests that lymphatics do not exist in deeper portions of the orbit. Second, the suffix "-oma" connotes neoplasm and thus rapid clonal expansion, which is uncharacteristic of these lesions. The more recently suggested nomenclature is "venous-lymphatic malformation."
In a recent clinical series of 1,264 consecutive patients, lymphangioma comprised 4 percent of space-occupying lesions in the orbit. Lymphangioma is classically a multilobulated cystic mass that can be found in both the intraconal and extraconal orbit. Typically, this malformation presents in childhood, though there are case reports of first presentations in the eighth and even ninth decades of life. Orbital lymphangioma becomes clinically apparent after hemorrhage occurs within the lesion, which may be spontaneous or secondary to trauma or surgery. In our patient, the use of a non-steroidal anti-inflammatory medication for the unrelenting headache may have actually caused a hemorrhage within the lesion, leading to the abrupt presentation.
Lymphangioma can appear in the orbit, eyelids or conjunctiva. Its natural history is such that if it does not bleed, its size can wax and wane slightly with upper respiratory infections, similar to other lymphoid tissue. It does not increase in size with Valsalva maneuver in contrast to orbital varices. MRI is superior to CT for soft tissue delineation and to track stages of bleeding. As blood ages, its paramagnetic properties change, and thus lymphangioma can take on a heterogeneous appearance.
The complications of orbital lymphangioma include hyperopia or astigmatism from globe deformity, as well as strabismus and resulting amblyopia. The above case demonstrates how proptosis may cause ocular surface disease. Exposure keratopathy, corneal ulcers and even corneal perforation can result. Other sequelae include optic neuropathy and retinal vascular occlusions.
The management of orbital lymphangioma is challenging. Surgery is difficult because of the friable nature of these cysts and their propensity for profuse bleeding. Also, despite aggressive intervention, they can recur. If the lesion is stable, observation with periodic imaging is reasonable.
If there are vision-threatening complications or cosmetic concerns, surgery is indicated. Depending upon presentation, partial or total surgical debulking is performed. Other surgical approaches include drainage with needle aspiration or bony decompression. Some surgeons use adjuncts such as carbon dioxide lasers to shrink the malformations or polymers such as fibrin glue to harden them for easier removal. Other experimental interventions, which avoid radical debulking but reduce the burden of the lesion, involve injection of sclerosing agents to incite endothelial damage or modified biologic agents to invoke lymphocytotoxic activity.
Dr. Sobel would like to thank Carol Shields, MD, and Brian Marr, MD, of Wills Eye Institute Ocular Oncology for their assistance with this case. Photos/Imaging courtesy of Wills Eye Oncology Service,
Bibliography
Bailey ST, Wojno TH, Shields CL, Grossniklaus HE. Late onset presentation of orbital lymphangioma. Ophthal Plast Reconstr Surg 2007;23:100-3.
Boulos PR., Harissi-Dagher M, Kavalec C, Hardy I, Codere F. Intralesional injection of tisseel fibrin glue for resection of lymphangiomas and other thin-walled orbital cysts. Ophthal Plast Reconstr Surg 2005;21:171-6.
Gunduz K, Demirel S, Yagmurlu B, Erden E. Correlation of surgical outcome with neuroimaging findings in periocular lymphangiomas. Ophthalmology 2006; 113: 1231-1236.
Harris GJ. Orbital Vascular Malformations: A consensus statement on terminology and its clinical implications. Orbital Society. American Journal of Ophthalmology 1999;127:453-5.
Rootman J. Disease of the orbit: A multidisciplinary approach. Lippincott W&W: 2nd edition. 2003. pp 522-528.
Schwarcz RM, Ben Simon GJ, Cook T, Goldberg, RA. Sclerosing therapy as first line treatment for low flow vascular lesions of the orbit. Am J Ophthalmol 2006;141:333-9.
Shields JA, Shields CL, Scartozzi R. Survey of 1,264 patients with orbital tumors and simulating lesions: The 2002 Montgomery Lecture, part 1. Ophthalmology 2004;111:997-1008.