A 2-year-old Caucasian male was referred to the Wills Eye Institute Department of Pediatric Ophthalmology and Ocular Genetics by an outside physician for evaluation of high myopia and the presence of nystagmus. The onset of nystagmus occurred at 2 months of age. He had been wearing spectacles since he was 7 months, with improvement of both his visual acuity and nystagmus.
Medical History
The pregnancy was uneventful and he was born full-term by spontaneous vaginal delivery. The patient had no prior surgeries, no hospital admissions and no serious injuries. Notably, a cystic area on the occiput of the skull was discovered on fetal ultrasound. A postnatal CT was performed and no communication was found between the intracranial vault and the elevated occipital lesion. Family history and pedigree revealed no evidence of parental consanguinity or a constricted gene pool. A maternal uncle reportedly had very fair skin, an inability to tan and high myopia without nystagmus. A maternal great aunt had severe developmental delay.
Examination
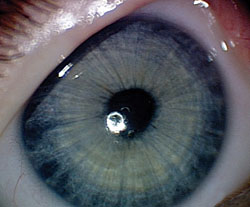
General examination of the patient revealed a fair-skinned, blue-eyed child with blond hair, mild mid-facial hypoplasia, and an elevated area of alopecia at the occiput (See Figure 1). Ophthalmic examination revealed a cycloplegic refraction of -21.50 +3.00 X 90 in the right eye, and -23.50 +2.00 X 75 in the left. The pupils were equal, round and reactive, without a relative afferent pupillary defect. Extraocular muscle motility was full, with horizontal, symmetrical, pendular nystagmus and an additional latent component in each eye. There was a preference for a 5 to 10 degree chin down position, with a right head tilt. There was also an exotropia of 18 prism diopters at distance, and 20 diopters at near. Intraocular pressure was 11 mmHg in the right eye and 14 mmHg in the left eye. Slit-lamp examination of the anterior segment was significant for cryptless irides with radial furrows and no transillumination defects (See Figure 2).
|

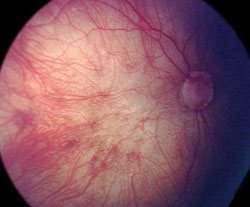
Dilated fundus examination (See Figure 3) of the right eye revealed abnormal fibrillar condensations in the vitreous, anomalous optic nerves, bilateral poor foveal reflexes, and diffuse retinal attenuation with a prominent choroidal pattern. There was a geographic area of macular atrophy. Pigmentary mottling was present 360 degrees around the midperiphery. There was no evidence of retinal breaks, retinal tears or lattice degeneration.
What is your differential diagnosis? What further workup would you pursue?
- See more at: http://www.revophth.com/content/d/wills_eye_resident_case_series/i/2417/c/41029/#sthash.x427xWBf.dpufWhat is your differential diagnosis? What further workup would you pursue?
- See more at: http://www.revophth.com/content/d/wills_eye_resident_case_series/i/2417/c/41029/#sthash.x427xWBf.dpufWhat is your differential diagnosis? What further workup would you pursue?
- See more at: http://www.revophth.com/content/d/wills_eye_resident_case_series/i/2417/c/41029/#sthash.x427xWBf.dpufWhat is your differential diagnosis? What further workup would you pursue?
What is your differential diagnosis? What further workup would you pursue?
- See more at: http://www.revophth.com/content/d/wills_eye_resident_case_series/i/2417/c/41029/#sthash.x427xWBf.dpufWhat is your differential diagnosis? What further workup would you pursue?
- See more at: http://www.revophth.com/content/d/wills_eye_resident_case_series/i/2417/c/41029/#sthash.x427xWBf.dpuf


