The differential diagnosis included inadequate treatment of bacterial keratitis, fungal keratitis, acanthamoeba keratitis and atypical mycobacteria keratitis. The patient opted to undergo corneal culture, while starting fortified tobramycin and cefazolin every hour around the clock, and scopolamine twice daily. On follow-up three days later, the vision in the left eye decreased to count fingers at 1 foot, and the anterior examination revealed a new, 1.4 x 1.4 mm epithelial defect, with the infiltrate increasing to 2.0 x 3.1 mm, and a new hypopyon of 0.5 mm.
The corneal culture did not demonstrate any growth. However, given the suspicion for fungal infection, topical voriconazole 1% was started. Four days later, his vision further decreased to hand motion. His epithelial defect had resolved, but the hypopyon increased to 1 mm and the infiltrate remained. His intraocular pressure increased to 24 mmHg. At this time, additional treatment for fungal keratitis was initiated with oral voriconazole, and IOP-lowering agents were started. Despite this aggressive therapy he failed to improve.
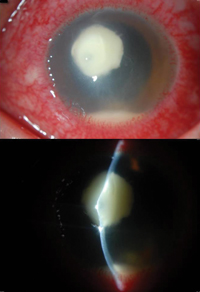
Given the lack of improvement he underwent intrastromal injection of voriconazole. Five small aliquots of voriconazole (50 micrograms in 0.1 ml) were injected into the mid-stroma using a 27-ga. needle to surround the infiltrate. The total dose was approximately 0.10 to 0.15 ml. Amphotericin drops once every two hours around the clock were added. Several days later, examination revealed an area of corneal thinning and cystic bulging at the center of the infiltrate, signaling impending perforation (See Figure 2). The following day, the patient underwent an urgent penetrating keratoplasty, with half the corneal button sent to pathology and half the corneal button sent to microbiology. He continued the topical and oral voriconazale and topical amphoteracin.
|

Discussion
Fungal keratitis is more commonly seen in developing nations and tropical climates. Annual incidence in North America is approximately 1,500 cases per year.1 Common fungal organisms can be divided into filamentous and non-filamentous. The most common filamentous fungi include Fusarium and Aspergillus species. In North America, the most common cause of fungal keratitis is the yeast Candida. Risk factors for filamentous fungal infection include trauma, especially if plant matter is involved. Non-filamentous organisms are more commonly seen in patient with diabetes and other immunocompromised states. Signs of fungal infection which may differentiate it from bacterial infection include feathery borders with satellite lesions, and deep stromal and anterior chamber invasion. Progressive corneal thinning or perforation may occur in the setting of unrecognized and thus improperly treated ulcers.
The diagnosis of fungal keratitis is often delayed, as it may be difficult to recognize and is often initially treated as a bacterial infection. For patients with the above risk factors who do not improve on topical antibiotics, especially fortified agents, fungal etiologies should be suspected. Corneal scraping for smears and cultures, including for fungus, should be obtained. Corneal biopsy can also be considered if scrapings fail to help determine the causative agent. Biopsy can be up to 83 percent sensitive in identifying the pathogen.2
The antifungal agents most commonly used to treat fungal keratitis include polyenes, azoles and pyrimidine analogues. Polyenes such as amphotericin and natamycin bind ergosterol, leading to interference with fungal cell membrane synthesis. Azoles interfere with cell membrane formation through a different method of action by inhibition of cytochrome P450. Azoles include voriconazole, itraconazole, fluconazole and miconazole. Flucytosine is an antimetabolite pyrimidine analogue, which is less commonly used.
Various randomized controlled studies have been conducted to compare the efficacy of different antifungals, and all have enrolled patients in developing countries. According to a recent Cochrane review of the literature, there is no conclusive evidence in favor of any one agent.3 Multiple agents as well as methods of administration have been compared with each other, generally without any observed difference in outcome.4-9 However, the recent Mycotic Ulcer Treatment Trial (MUTT) did demonstrate results in favor of topical natamycin over vorico-nazole for one organism. For cases of Fusarium keratitis, natamycin use resulted in a significantly decreased rate of perforation compared with voriconazole use (odds ratio of 0.06).10 While the MUTT study is the only large scale, randomized control trial for fungal keratitis that showed statistical significance for commonly used agents, it must be emphasized that all patients were enrolled in South India, and no contact lens wearers were included.
In developed countries such as the United States, a large proportion of fungal infection is contact lens-related or found in patients severely immunocompromised. Therefore, generalizations must be made cautiously. First-line antifungal agent selection in the absence of culture data should be made considering the mechanism of infection as well as the suspected organism. Subconjunctival, intrastromal, as well as intracameral agents have also been used with variable success, and without large head-to-head comparison trials. In particular, intrastromal voriconazole has been shown to be beneficial as an adjunctive therapy to topical natamycin.9 In patients with systemic fungemia, infectious disease consultation should be obtained. For patients who are candidates for topical monotherapy, natamycin 5% is the only commercially available agent while other agents must be mixed at compounding pharmacies or in the clinic.
For patients who fail medical therapy and progress to impending or frank perforation, as in our patient, an urgent penetrating keratoplasty is often the next step. Two studies from China have examined outcomes following penetrating keratoplasty in this setting.11,12 Recurrence rates ranged from 6 to 7 percent, while the cure rate was over 80 percent. However, there was a high rate of rejection of approximately 30 percent, likely secondary to the avoidance of topical steroids in the immediate postoperative setting. In these studies, steroids were only considered starting at two weeks if the eye was healing well and exhibited no significant inflammation. Risk factors for recurrence include hypopyon, perforation or limbal and lens involvement.
In summary, fungal keratitis is a vision-threatening problem that is important to diagnose early. While natamycin is the only commercially available topical agent, many agents and methods of administration are available to the cornea specialist. For ulcers that are resistant to initial medical therapy, early referral may be necessary for further intervention, and possible surgical treatment. REVIEW
The author would like to thank Christopher J. Rapuano, MD, and Dr. Ralph C. Eagle Jr., MD, for their help in preparing this case.
1. Thomas PA, Kaliamurthy J. Mycotic keratitis: Epidemiology, diagnosis and management. Clin Microbiol Infect 2013;19(3):210-20.
2. Alexandrakis G, Haimovici R, Miller D, Alfonso EC. Corneal biopsy in the management of progressive microbial keratitis. Am J Ophthalmol 2000;129(5):571-6.
3. FlorCruz NV, Peczon IV, Evans JR. Medical interventions for fungal keratitis. Cochrane Database Syst Rev 2012;2:CD004241.
4. Agarwal PK, Roy P, Das A, Banerjee A, Maity PK, Banerjee AR. Efficacy of topical and systemic itraconazole as a broad-spectrum antifungal agent in mycotic corneal ulcer. A preliminary study. Indian J Ophthalmol 2001;49(3):173-6.
5. Prajna NV, John RK, Nirmalan PK, Lalitha P, Srinivasan M. A randomised clinical trial comparing 2 percent econazole and 5 percent natamycin for the treatment of fungal keratitis. Br J Ophthalmol 2003;87(10):1235-7.
6. Mahdy RA, Nada WM, Wageh MM. Topical amphotericin B and subconjunctival injection of fluconazole (combination therapy) versus topical amphotericin B (monotherapy) in treatment of keratomycosis. J Ocul Pharmacol Ther 2010;26:281-5.
7. Prajna NV, Mascarenhas J, Krishnan T, et al. Comparison of natamycin and voriconazole for the treatment of fungal keratitis. Arch Ophthalmol 2010;128:672-8.
8. Arora R, Gupta D, Goyal J, Kaur R. Voriconazole versus natamycin as primary treatment in fungal corneal ulcers. Clin Experiment Ophthalmol 2011;39(5):434-40.
9. Sharma N, Chacko J, Velpandian T, et al. Comparative evaluation of topical versus intrastromal voriconazole as an adjunct to natamycin in recalcitrant fungal keratitis. Ophthalmology 2013;120:677-81.
10. Prajna NV, Krishnan T, Mascarenhas J, et al. The mycotic ulcer treatment trial: A randomized trial comparing natamycin vs voriconazole. JAMA Ophthalmol 2013;131:422-9.
11. Shi W, Wang T, Xie L, et al. Risk factors, clinical features, and outcomes of recurrent fungal keratitis after corneal transplantation. Ophthalmology 2010;117:890-6.
12. Xie L, Dong X, Shi W. Treatment of fungal keratitis by penetrating keratoplasty. Br J Ophthalmol 2001;85(9):1070-4.


