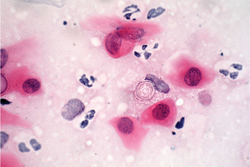
After examination of the right eye the patient was thought to have a bacterial ulcer with a component of medicamentosa from his multiple topical treatments. However, once the pseudo-dendritic staining and subepithelial infiltrates were noted in the asymptomatic left eye, suspicion was raised for Acanthamoeba keratitis. Both eyes were re-cultured for bacteria and fungi, corneal scrapings from both eyes were sent for pathology, and the patient’s contact lens case was sent for cultures. Polymyxin/bacitracin ophthalmic ointment every two hours was started in the right eye. Two days later pathology results were reported positive for Acanthamoeba in both eyes (See Figure 4). Corneal cultures and contact lens case cultures were negative. The patient was started on dual therapy with polyhexamethylene biguanide (PHMB) and propamidine (Brolene) drops every hour around the clock in both eyes.
|
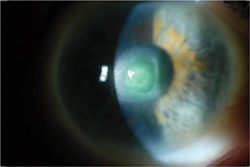
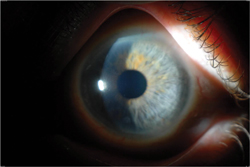
The patient had a slow improvement on this treatment regimen (See Figures 5 & 6). The medications were gradually tapered and the patient received a five-month course of treatment in the right eye and a four-month course of treatment in the left eye. Visual acuity in the right eye after treatment remained 20/200 due to central corneal scarring, while in the left eye, visual acuity after treatment was 20/20.
Discussion
Acanthamoeba keratitis is an infection of the cornea caused by cyst-forming protozoans ubiquitous in the environment.1 The condition was first described in the early 1970s but an increase in incidence occurred in the 1980s associated with an increase in soft contact lens wear.2 The most well-known and strongest risk factor for Acanthamoeba keratitis is contact lens wear, as well as inadequate lens disinfection.1-3 Additional risk factors in contact lens wearers include swimming in lenses, overnight wear of lenses and exposure of lenses to contaminated water and well water.4 Other risk factors that disrupt the normal epithelial barrier of the cornea include minor corneal trauma and epithelial basement membrane dystrophy; dry eye may also predispose to disease.1-3
Acanthamoeba keratitis is often initially misdiagnosed as herpetic or bacterial disease, leading to delay in initiation of appropriate treatment.4,5 Clinical features of Acanthamoeba keratitis include pain out of proportion to clinical signs, photophobia and tearing.1 Absence of pain does not, however, preclude the diagnosis. Early in the course of the disease, a pseudo-dendritic epitheliopathy, subepithelial infiltrates and radial keratoneuritis may be noted.1,4 Our patient in this case demonstrated the early Acanthamoeba keratitis paradigm in his asymptomatic left eye. Of note, although this eye was clearly involved, the patient was without pain in his left eye. Later disease is characterized by ring infiltrates, ulceration, keratic precipitates and sometimes hypopyon formation, demonstrated by our patient’s symptomatic right eye.1,4 Prompt diagnosis and treatment initiation is important in Acanthamoeba keratitis because early treatment leads to better visual outcomes.4,5
Definitive diagnosis of Acanthamoeba keratitis can be made only with cultures or histology of corneal scrapings as in our case.2 Confocal microscopy is used in some centers to aid in diagnosis, with reported sensitivity in one study of 90.6 percent and specificity of 100 percent.6 If clinical suspicion for Acanthamoeba keratitis warrants, however, treatment should not be delayed pending definitive diagnosis.
Treatment of Acanthamoeba keratitis is aimed at killing the cystic, or dormant, form of the organism, which is highly resistant to most treatments and can persist for months to years.1,2 Two classes of medication have activity against Acanthamoeba cysts: biguanides and diamidines. These medications are not commercially available in the United States and can only be obtained from compounding pharmacies or from overseas. The two biguanides currently in use are polyhexamethylene biguanide (PHMB) 0.02% and chlorhexidine 0.02%. These agents act by disrupting the cytoplasmic membrane of Acanthamoeba trophozoites and cysts resulting in cell death.1 The diamidines include propamidine (Brolene) 0.1% and hexamidine 0.1% and also work through increasing membrane permeability in both trophozoites and cysts.1 Treatment may be initiated with either a biguanide alone or a biguanide in addition to a diamidine and is typically prescribed every hour around the clock for the first few days of treatment. Practice patterns vary by provider as there are no studies demonstrating efficacy of dual therapy over monotherapy.7 Our patient was initially started on dual therapy with PHMB and propamidine but due to propamidine toxicity finished out his course on PHMB alone. His overall course of five months in one eye and four months in the other eye is typical, as most patients require several months of treatment prior to resolution.2
Acanthamoeba keratitis is a challenging disease to diagnose and to treat. As early diagnosis and treatment portends a better visual prognosis, Acanthamoeba must be considered in any patient thought to have herpetic epithelial disease, contact lens-related subepithelial infiltrates or a corneal ulcer unresponsive to treatment. REVIEW
The author would like to thank Christopher Rapuano, MD, and Ralph Eagle Jr., MD, for their assistance in preparing this case.
1. Dart JK, Saw VP, Kilvington S. Acanthamoeba keratitis: Diagnosis and treatment update 2009. Am J Ophthalmol 2009;148: 487-499.
2. Hammersmith KM. Diagnosis and management of Acanthamoeba keratitis. Curr Opin Ophthalmol 2006 Aug; 17(4): 327-31.
3. Page MA, Mathers WD. Acanthamoeba keratitis: A 12-year experience covering a wide spectrum of presentations, diagnoses, and outcomes. J Ophthalmol. 2013 Published online 2013 Jun 12.
4. Thebpatiphat N, Hammersmith KM, Rocha FN, Rapuano CJ, Ayres BD, Laibson PR, Eagle RC Jr., Cohen EJ. Acanthamoeba Keratitis: A Parasite on the Rise. Cornea 2007;26:701-706.
5. Chew HF, Yildiz EH, Hammersmith KM, Eagle RC Jr, Rapuano CJ, Laibson PR, Ayres BD, Jin YP, Cohen EJ. Clinical Outcomes and Prognostic Factors Associated With Acanthamoeba Keratitis. Cornea 2011;30:435-441.
6. Tu EY, Joslin CE, Sugar J et al. The relative value of confocal microscopy compared to superficial corneal scrapings in the diagnosis of acanthamoeba keratitis. Cornea 2008;27:764-767.
7. Oldenburg CE, Acharya NR, Tu EY, et al. Practice patterns and opinions in the treatment of acanthamoeba keratitis. Cornea 2011;30:1363-8.


