When evaluating candidates for CK or conductive keratoplasty (Refractec, Irvine, Calif.), there is an additional factor to consider. In our experience, we have learned that CK is not a typical correction for monovision. The treatment creates a more prolate cornea, providing patients with a larger depth of field than we've previously seen with other surgical presbyopic corrections. With NearVision CK, the most recent advance in the technique, patients achieve a significant improvement in their near vision, while also showing a high satisfaction rate with their distance vision.
In an analysis of the effect of NearVision CK on the cornea, Houston surgeon Jack Holladay concluded that the procedure increases the central power of the cornea, creating a more prolate shape, although there is slightly less of an increase in power in the exact central 1 mm. Dr. Holladay analyzed corneas treated with NearVision CK and found that the procedure produces a multifocal-modified, prolate surface that utilizes the pupil and the shape of cornea to yield, on the average, a two-line reduction in distance (20/20 to 20/30) with a gain of seven to nine lines at near (20/200 to 20/25).
It's a trade-off that patients enrolled in the NearVision CK Food and Drug Administration clinical study were happy with—84 percent of patients at one year reported that they were satisfied or very satisfied with the results of the surgery, while 100 percent said the quality of depth perception was fair to excellent.
A Better Way
As a result, we've come to realize that the standard trial of a spherical contact lens on the non-dominant eye simply does not adequately give patients an idea of what their post-CK vision will be like. This is why we now perform a one- to two-week trial of a multifocal contact lens in the non-dominant eye to more realistically demonstrate to prospective patients what their vision will be like after NearVision CK.
I fit patients with a multifocal contact lens choosing a power that is +0.50 to +0.75 D over the best corrected vision with the low near add. I decided on using a multifocal contact lens through a prospective study to compare results when patients were fitted with the multifocal contact lens or a standard spherical lens.
Clinical Results
In this study, 10 patients were randomized into two groups following standard visual acuity measurements, as well as wavefront aberrometry. Five of the patients were fitted with a monovision contact lens in their non-dominant eye. The lens we used was +1.5 D over the BCVA. The second group received the multifocal contact lens. After fitting, we repeated the same visual acuity and wavefront tests.
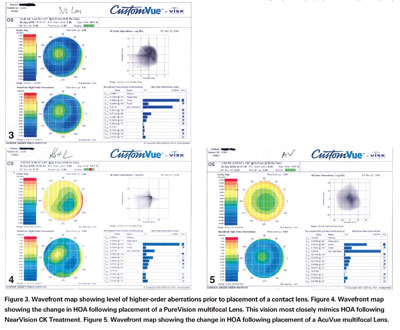
Figure 3. Wavefront map showing level of higher-order aberrations prior to placement of a contact lens. Figure 4. Wavefront map showing the change in HOA following placement of a PureVision multifocal Lens. This vision most closely mimics HOA following NearVision CK Treatment. Figure 5. Wavefront map showing the change in HOA following placement of a AcuVue multifocal Lens.
The findings were very interesting. In the monovision group, the average loss of distance vision was four lines, while the average loss of distance vision in the multifocal group was an average of one line. Improvement in near vision was the same in both groups—an average of four lines.
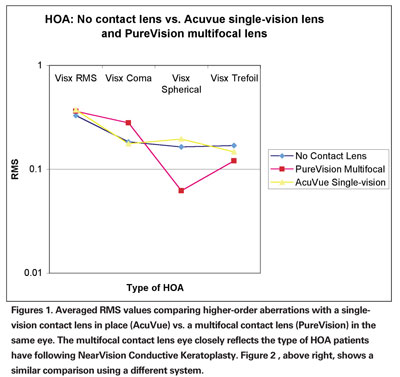
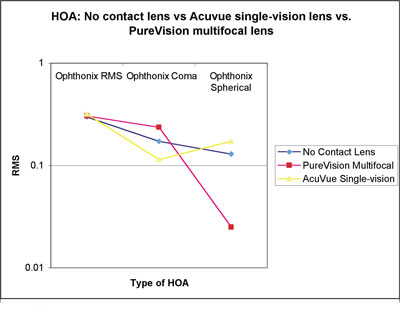
The wavefront results showed that the monovision contact lens eyes had a mean total aberration measurement (RMS) of 0.37 µm, while the multifocal contact lens eyes had a mean of 0.36 µm. The mean HOA in the uncorrected eyes was 0.33 µm. The multifocal eyes had a higher level of coma, 0.28 µm, compared to 0.18 µm in the uncorrected and monovision eyes. The mean amount of spherical aberration was lowest in the multifocal eyes, with 0.06 µm, compared to 0.18 µm for the monovision contact lens eyes. Interestingly, these results are the same as what we see when wavefront aberrometry is measured on post-CK eyes. Figures 1 and 2 show the average difference in HOA between the single-vision lens and the multifocal with measurements done on an AMO/Visx aberrometer, as well as an Opthonix aberrometer. Figures 3, 4 and 5 show how the HOAs change in one patient's eye when the single-vision lens is in place, and then with the multifocal contact lens.
This clinical study, while small, demonstrates the benefits of fitting potential NearVision CK patients with a multifocal contact lens rather than a standard monofocal lens. Educating patients about the benefits of NearVision CK has been challenging, particularly plano presbyopes. Due to their visual requirements, a trial of monovision contact lenses has generally not been successful in convincing patients to undergo the procedure.
In our practice, we have found a better way by using the multifocal contact lens in the non-dominant eye and slightly over-plussing the patient. It provides them with a vision that is much closer to the results we see with NearVision CK. As important, the results obtained with the multifocal lens very closely match post-CK vision, right down to the higher-order aberrations.
This strategy has improved our conversion rate and allows us to help more patients reduce their reliance on glasses for near and intermediate tasks.
Drs. Geffen and Gordon practice at Gordon, Binder & Weiss Vision Institute, in La Jolla. Dr. Geffen is an adjunct clinical professor at the Illinois College of Optometry. Contact him at DIG2020@aol.com.



