A challenge for many ophthalmologists is the diagnosis and treatment of lower eyelid malpositions. Whether an eyelid is in-turning or out-turning, patients complain of ocular irritation, foreign body sensation, tearing, decreased vision and an abnormal eyelid appearance. However, the underlying reason for each of these complaints is different in each scenario.
For the outturned eyelid, ocular irritation, foreign body sensation and decreased vision are often caused by ocular exposure and drying. Tearing in ectropion is usually due to decreased lacrimal pump function, since proper tear drainage requires normal eyelid positioning against the globe. For entropion, the irritation and vision changes are caused by direct rubbing of the eyelashes or eyelid skin against the ocular surface. Tearing is secondary to these issues in the in-turning eyelid.
To understand how eyelid malpositions occur, one must have a grasp of the forces acting on an eyelid and in particular those that keep an eyelid in its normal position. Here is a quick review.
Forces Acting on the Lid
The lower eyelid is acted upon in four directions—away from the globe or outwards, towards the globe or inwards, superiorly and inferiorly. Figure 1 summarizes these forces. Forces which push the eyelid outward include gravity, the lower eyelid retractors, and the eyeball itself. Forces pulling the eyelid towards the eyeball include the canthal tendons and the orbicularis muscle. Forces elevating the eyelid include the orbicularis, while forces pulling the eyelid down include gravity and the lower eyelid retractors. Normal eyelid position is accomplished when these forces are in balance. A change in these forces can cause a malposition. For example, lateral canthal tendon weakening will decrease the eyelid force towards the eye leading to ectropion (See Figure 2, below). With this basic understanding of forces acting on the lower eyelid, we can now differentiate why eyelid malpositions occur. This is summarized in Table 1.
Interventions for lower eyelid malpositions should address the underlying cause. In the example above, a weakened lateral canthal tendon causing ectropion can be strengthened via surgical tightening or resuspending. However medical and surgical interventions for lower eyelid malpositions are limited. The two main medical interventions for eyelid malpositions include Botox and tissue fillers. Botox can be used to weaken a muscle to help balance forces causing eyelid malposition. For example, spastic entropion is due to an overactive orbicularis muscle, often due to ocular irritation or inflammation. Besides treating the irritation or inflammation, Botox can be used to weaken the offending muscles, rebalancing the forces, and restore normal eyelid position. Fillers can also be used in cases of eyelid malposition. A cause of ectropion can be a weak orbicularis secondary to facial nerve palsy. Injection of tissue filler can serve as a bolster or spacer to "hold up" the eyelid, strengthening the relative force of the orbicularis and restoring eyelid positioning. However in both cases, medical interventions are usually temporizing.
Surgical interventions involve either lengthening tissues either with grafts or spacers or shortening/tightening tissues for a more permanent result. Surgical grafting is very helpful in cicatricial disease; contracture of the conjunctiva or posterior lamella of the eyelid causes increased forces inward or entropion. Likewise, anterior lamellar scarring from prior trauma or actinic changes will cause ectropion. In each case, lengthening the scarred tissue with a tissue graft (skin for the outer lamella, mucus membrane for the inner lamella) will allow the eyelid to resume its normal position. Tightening the canthal tendons or the lower eyelid retractors can also help reposition an eyelid in the case of laxed or weakened tissue. Involutional entropion is often caused by dehiscence or weakening of the lower eyelid retractors (See Figure 3); surgical advancement or tightening of the lower eyelid retractors can restore normal eyelid function.
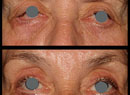
Finally, a combination of tightening one tissue and grafting another tissue is of benefit in complex cases. A patient with facial nerve palsy will have both ectropion and lid retraction, causing exposure symptoms. A combination of lateral canthal tightening via lateral tarsal strip surgery (See Figure 4) and posterior lamellar grafting with ear cartilage can be helpful in improving eyelid closure.
In summary, identifying the underlying cause of a malpositioned eyelid will aid treatment and ultimately lead to restored eyelid and ocular function.
Dr. Bernardino is at the Yale School of Medicine, Department of Ophthalmology, Section of Ophthalmic Plastics and Orbital Surgery. Contact him at