A 41-year-old man presented with one week of progressively worsening vision in the right eye, described as a black band across his visual field, and one day of vision loss in the left eye. The patient denied any other complaints on review of systems including rash, joint pain, recent illness, diarrhea, numbness, weakness, shortness of breath and chest pain. One year prior to presentation the patient had a painless penile lesion described as a pimple with some ulceration, which resolved on its own. He then developed bilateral tinnitus prior to changes in vision.
Medical History
Past medical history was significant for syphilis, treated seven years earlier with intramuscular penicillin, and hyperthyroidism. He denied chronic medication use.
Examination
The patient’s vital signs were stable and within normal limits. Ocular examination demonstrated a best corrected visual acuity of 20/400 OD and 20/20 OS. External examination was within normal limits. Pupillary exam showed no anisocoria and no relative afferent pupillary defect. Extraocular motility was full in both eyes. Visual fields were full to confrontation OU.
 | 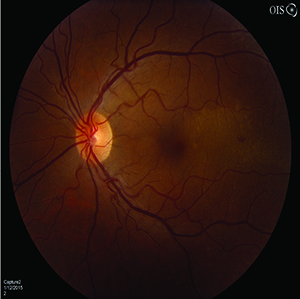 | 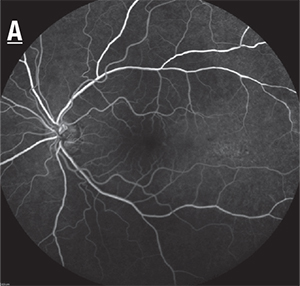 |
| Figure 1a. Fundus photograph OD showing circular, yellow, placoid lesions in the fovea and temporal macula. Figure 1b. Fundus photograph OS showing similar yellow placoid lesions, as well as a small area of retinal hemorrhage in the temporal macula. | Figure 2a. Early-phase fluorescein angiography OS showing speckled hypofluorescence and scattered hyperfluorescence in the area of the placoid macular lesions. | |
Slit-lamp examination revealed 0.5+ anterior chamber cell and 1+ vitreous cell bilaterally, without conjunctival injection or posterior synechiae. Intraocular pressure was 14 mmHg OU. Fundoscopic examination of the right eye exhibited yellow, circular, placoid lesions in the macula bilaterally (See Figure 1a, 1b).
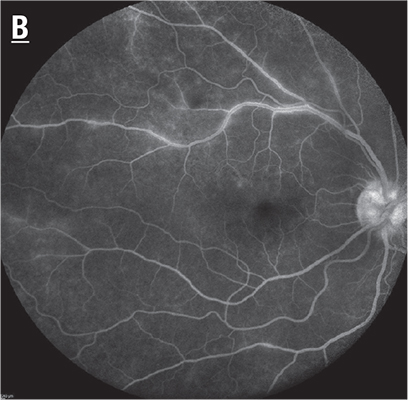 | Figure 2b. Venous laminar-phase FA OD showing punctate hyperfluorescence surrounding the retinal vasculature. |
 | |
| Figure 3a (top). Raster SD-OCT of the right eye demonstrating retinal pigment epithelium nodularity and inner segment-outer segment disruption with preserved foveal depression. The left eye demonstrated similar findings. Figure 3b (bottom). SD-OCT line scan OD demonstrating retinal pigment epithelium nodularity. The left eye demonstrated similar findings. | |
Imaging
Fluorescein angiography showed early punctate hypofluorescence with persistent mid to late hyperfluorescence in both eyes (See Figure 2a, left, and 2b, above). Spectral-domain optical coherence tomography demonstrated disruption of the junction with retinal pigment epithelium nodularity (See Figure 3a, 3b, above).
What is your differential diagnosis? What further workup would you pursue?
Please click this link for diagnosis, workup, treatment and discussion.
Please click this link for diagnosis, workup, treatment and discussion.


