Over the years, questions have been raised about the viability of refractive lens exchange for high myopes. Some physicians think it’s acceptable, while others feel it’s too great a risk, due to the incidence of retinal detachment in these particular patients. Here’s a look at some of the current perspectives on RLE in the high myope.
 |
|
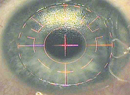
In a highly myopic eye, the anterior chamber can get overly deep. The fix for this is breaking the reverse pupillary block by lifting the iris.
(Images courtesy Uday Devgan, MD) |
Alicante, Spain, surgeon Jorge Alio studied the incidence of retinal detachment in 439 eyes of 274 high myopes who had lens surgery, both RLE and cataract. The average age of the patients was 62.2 years (range: 21 to 90). The average follow-up was 62 months (range: two to 147 months).1 The researchers divided the patients into two groups based on age: Group 1 comprised patients 50 years and younger; Group 2 patients were older than 50. They also stratified eyes by axial length (28 mm or shorter in 274 eyes, longer than 28 mm in 165 eyes). The physicians found that the overall incidence of retinal detachment in the eyes was 2.7 percent. The average age of patients with RD was 56, the average length of their eyes was 27.85 mm and the average refraction was -13.4 D. In Group 1, the younger patients, the risk of RD was 3.65 percent, vs. 2.5 percent in the older group.
Dr. Alio’s study’s findings are similar to a large study from Germany of 2,356 cataract surgeries in high myopes. This study found an absolute incidence of RD ranging from 1.5 percent to 2.2 percent, but the researchers noted that the risk for detachment was significantly higher in younger patients.2
Though Dr. Alio says his group found a trend toward a higher risk for RD in patients younger than 50, he notes that it wasn’t statistically significant. He adds that even large studies haven’t definitively shown the actual risk of RD in RLE because of the larger number of patients that would be necessary. However, he feels the trend he found is clinically significant when making judgment calls for these patients. “Patients under age 50 with axial lengths longer than 28 mm have a higher risk for retinal detachment,” says Dr. Alio. “The reason for this is the detachment of the vitreous following cataract surgery, which eventually leads to the complication. As there is no specific and reproducible way to see the vitreous in the high myope, especially the very high myope, my advice is to not perform refractive lens exchange in these myopic patients less than 55 years of age unless there’s clear evidence of a vitreous detachment.”
Chicago surgeon Parag Majmudar says that surgery can increase the risk for a retinal complication in these patients, though modern techniques may change that. “These high myopes all have thin retinas,” he says. “This is especially true where the vitreous base attaches. So any disturbance in the vitreous base can lead to retinal problems. There can be issues during surgery in which the shockwaves caused by a moving capsule get propagated posteriorly, causing traction on the vitreous base, which then causes a tear in the retina. However, I think this was more of an issue in the past with surgeons operating through larger incisions, where there may have been more bouncing of the anterior chamber, which caused more shockwaves to propagate through the vitreous. Now, surgeons are operating through 2- or 3-mm incisions, there aren’t as many chamber fluctuations during surgery and our phaco technology has improved to the point that there probably isn’t as much of a shockwave from it. There are a lot of positives with our current techniques.” Overall, surgeons say the risk factors they take note of are younger age, higher degrees of myopia, an absence of a posterior vitreous detachment and male sex.
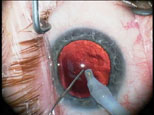 |
| Injecting viscoelastic with the non-dominant hand before removing the phaco probe from the eye can help keep the anterior chamber from collapsing. |
With the advent of toric and multifocal IOLs, surgeons say RLE is an attractive option for high myopes who may be presbyopic but not old enough to have developed a cataract, since phakic IOLs with these features aren’t yet on the market. These patients lie in what some surgeons say is a gray area: LASIK’s not going to be adequate to treat a high degree of myopia; the patient won’t want to wear contact lenses; he may be a little too old for phakic IOLs, based on their labeling; and he may not have any accommodation left. However, even though RLE can be an option for these patients, surgeons advise taking certain steps to ensure a good outcome.
“Make sure these patients have a good retinal exam beforehand, so any potential sources of retinal detachment can be treated,” says Dr. Majmudar. “When you’re operating on very high myopes, regardless of age, the main thing is to make sure your fluidics are such that the chamber isn’t bouncing up and down too much,” says Dr. Majmudar. “Use a smaller incision. And, though I haven’t had to do it a lot, it might be a good idea to put a suture at the close of the procedure in cases where there might potentially be a deep chamber in which there might be fluctuations postop. Also, make sure the bottle height isn’t too high, so you don’t have extra fluid coming in. In addition, you want to ensure that the eye is pressurized so that it’s not collapsing every time you come out.”
Los Angeles surgeon Uday Devgan, for whom RLE makes up about 10 to 15 percent of his IOL practice, agrees chamber maintenance is key. “When the capsular bag is completely empty and you’ve got all the cortex out, don’t just pull the I/A probe out of the eye, because doing so will allow the capsular bag to come forward and the vitreous base to shift. Instead, use your non-dominant hand to inject viscoelastic to fill up the capsular bag. It will help minimize the retinal traction.”
For Dr. Alio, choices of anesthesia and capsulorhexis size make a difference. “It’s important to avoid complications in these patients,” he says. “I only use topical anesthesia in order to avoid perforation of the globe, which is more frequent in very elongated eyes such as these, as well as to avoid posterior capsular disruption. For these reasons, I prefer a capsulorhexis of about 6 mm, no smaller. I use microincisional cataract surgery in order to avoid working inside the capsule—separating infusion and aspiration makes the fragments of the lens float and eliminates having to pick them up from the capsular bag—and I also use sedation to facilitate better control in cases where patients are very anxious.”
For patients just outside of the gray area, there are alternative procedures that can be effective, say surgeons. They say phakic IOLs might be an alternative in certain cases or, if the patient is less than -10 D, he could have LASIK or PRK. Some surgeons may also combine a lens procedure with a corneal laser surgery for very high myopes. However, if patients have any type of lens opacity, even a peripheral one, some physicians say they will lean toward a phakic lens or maybe RLE, taking into account their risk factors.
Though Dr. Majmudar says he’s not very aggressive with refractive lens exchange in very high myopes, he sees things moving more in that direction. “I see our approach moving that way since our technology and techniques have improved, both in terms of our surgery and the lenses we have to choose from,” he says. “In the future, I believe we’ll have more reasons to offer this as a viable option for patients.”
1. Alio JL, Ruiz-Moreno JM, Shabayek MH, et al. The risk of retinal detachment in high myopia after small incision coaxial phacoemulsification. Am J Ophthalmol 2007;144:93-8.
2. Neuhann IM, Neuhann TF, Heimann H, et al. Retinal detachment after phacoemulsification in high myopia: Analysis of 2,356 cases. J Cataract Refract Surg 2008;34:1644-57.