Three new options for presbyopia correction are currently under investigation: corneal inlays, scleral implants and laser procedures. Although these procedures are not yet FDA-approved for use in this country, they may soon become attractive alternatives for younger presbyopic patients who do not have cataracts or who desire a less-invasive procedure than refractive lens exchange.
“I think there is a place for a lot of different presbyopia surgeries. It’s not a one-size-fits-all thing,” says Barrie Soloway, MD, director of vision correction surgery at the New York Eye and Ear Infirmary.
Corneal Inlays
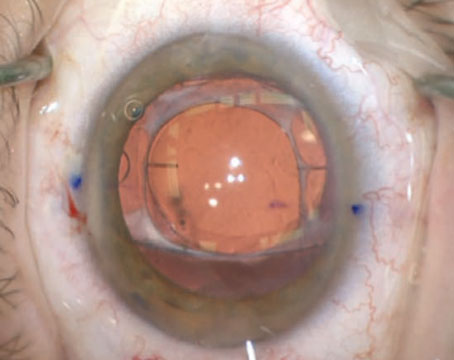
Currently, three different corneal inlays are under investigation. Each offers a different principle of action. The Kamra (AcuFocus, Irvine, Calif.) corneal inlay uses a pinhole effect. A recent study conducted in Turkey found that Kamra intracorneal inlay implantation is an effective, safe and reversible procedure for the long-term surgical treatment of presbyopia.1 This study included patients with emmetropic or post-LASIK presbyopia. Patients had an uncorrected near visual acuity of 20/40 or worse that was correctable to 20/25 or better at distance. The study included 39 patients aged 45 to 60 years, and at the four-year follow-up, all patients had two or more lines of improvement in uncorrected near visual acuity with no significant loss in distance vision. The mean final uncorrected near visual acuity was 20/20, and 96 percent of patients could read J3 or better. Uncorrected distance visual acuity was 20/40 or better in all eyes.
|

“Based on reports and presentations, near vision can be improved while retaining distance visual acuity with the Kamra presbyopic inlay,” says San Diego surgeon Steven Schallhorn, MD. “From limited data available for the other two inlays under investigation, it appears that they also improve near vision while retaining distance vision. But all of these presbyopic inlays represent a compromise. For the Kamra, light entering the eye is restricted, which may reduce contrast and night vision, and there can be optical side effects.”
He believes that patients who can adjust to monovision are more likely to tolerate an inlay. “Presbyopic inlays are only placed in one eye, and, similar to monovision, the near vision improvement is monocular. But unlike monovision, the inlay eye can retain distance vision,” Dr. Schallhorn says.
Two-year follow-up data from the clinical trial of the Kamra were reported at the ASCRS meeting. “The follow-up data showed that distance vision was preserved and averaged 20/20 in the inlay eye,” says Dan Durrie, MD, AcuFocus’ chief medical officer. “Near vision averaged J2, which is good enough to read without glasses. We saw some variability from patient to patient during the clinical study, and in analyzing the results, we did find that there was a difference depending on how the pocket was made for putting the inlay in, and some of the modern femtosecond lasers had better results than the early ones. So, internationally, now that it has been commercially approved, people are using the modern femtosecond lasers to create pockets in the cornea, and they are getting even better results than we saw in the clinical trials.”
Dr. Durrie, who is also in private practice with Durrie Vision in Overland Park, Kan., says placing the inlay is an easy procedure to perform. “Anyone who can do LASIK surgery has the capability of doing it, and surgeons seem to like the procedure.”
Another inlay under investigation is the PresbyLens (ReVision Optics, Lake Forest, Calif.), which is a 2-mm corneal inlay that is designed to improve near and intermediate vision by microscopically changing the shape of the eye’s surface. “The inlay is placed under a flap and creates a hyperprolate shape to the cornea, creating negative spherical aberration and an increased depth of field,” says Michael Gordon, MD, in private practice in La Jolla, Calif.
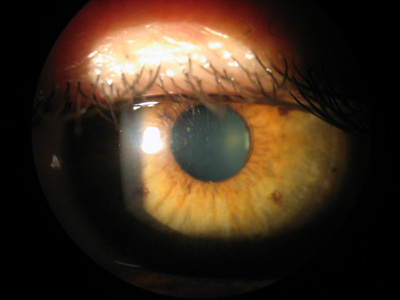
The third inlay is the Flexivue Microlens (Presbia, Los Angeles), which is a refractive inlay, according to Dr. Gordon. “This means that it has a different refractive index than the cornea. It has a central clear area surrounded by an area of add that can be varied according to patient needs. It works in a monovision situation in the non-dominant eye by providing add in that eye, and it is pupil-dependent,” he says.
One benefit of the inlays is that they are removable, so the effect is reversible. “If patients develop a cataract down the road, they have other options, and that just kind of makes it interesting, compared to having your lens replaced, which is not something that is removable. Another benefit is that it uses the same technology that everybody already has, so surgeons don’t have to go buy a new laser,” Dr. Durrie says.
Dr. Schallhorn believes that, in the future, an excimer laser procedure to target a specific refractive error will be performed along with an inlay to improve the results. “For instance, the Kamra inlay works on a depth of field principle using a small aperture,” he says. “If a patient has no refractive error and the inlay is implanted, distance vision will be retained, and there will be some near vision improvement. However, if the refractive error was slightly near-sighted, then the depth of focus range should provide better near vision while retaining distance vision. Targeting a very specific refractive error should result in better visual performance after the inlay.”
A recent study conducted in Japan found that simultaneous intracorneal inlay implantation and LASIK to treat presbyopia with emmetropia, hyperopia or myopia was safe and effective.3 This study included 360 eyes of 180 patients with a mean age of 52.4 years ±5.1. Patients had bilateral LASIK with simultaneous implantation of a corneal inlay in the non-dominant eye to treat presbyopia and ametropia. At the six-month postoperative visit, 64 patients were available for evaluation. Mean uncorrected near visual acuity in the eye with the inlay improved seven lines in hyperopic eyes, six lines in emmetropic eyes, and two lines in myopic eyes. Mean uncorrected distance visual acuity improved by three lines in hyperopic eyes, one line in emmetropic eyes, and 10 lines in myopic eyes.
Scleral Implants
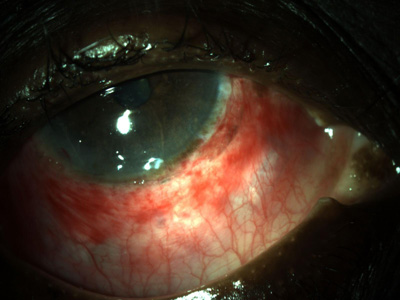
Another option that is currently under investigation is the PresVIEW scleral implant, which is a two-part clear plastic device that is approximately the size of a grain of rice.
“I’m pretty encouraged by the scleral implants because I like the fact that it’s not surgery on the visual axis. The implants are removable, and the effect is totally reversible,” Dr. Soloway says.
|
Laser Procedures
According to Dr. Schallhorn, monovision with an excimer laser remains popular among refractive surgeons. A recent study conducted in Spain found that monovision correction by LASIK improved functional near vision in presbyopic patients.4 However, although distance visual acuity was good, contrast sensitivity and stereoacuity diminished significantly. In this study, LASIK was performed with the Allegretto Wave Eye-Q 400 Hz laser. The dominant eye was corrected for distance vision, and the non-dominant eye was corrected for near vision by targeting -1.25 D of myopia. The study included 50 eyes of 25 patients with a mean age of 49.3 years ±4.5. Postoperatively, more than 90 percent of patients had a binocular uncorrected distance and near visual acuity of 0.0 logMAR or better. However, the contrast sensitivity function diminished, especially in the non-dominant eye and with binocular vision. All patients experienced significantly worse stereoacuity. Visual discrimination capacity declined in non-dominant eyes and under binocular conditions. No significant changes occurred in dominant eyes.
Additionally, presbyLASIK and a femtosecond laser procedure called Intracor (Technolas, St. Louis) are under investigation. Neither is currently FDA-approved for use in the United States. “Intracor works by creating concentric rings in the cornea centrally to weaken the central cornea so you get a push forward, creating a hyperprolate shape,” Dr. Gordon says. “Hopefully, we are going to have a group of procedures that will be available, and then we, as surgeons, will have to decide which procedure is going to be best for a given individual based on whether he has a refractive error, the patient’s age, the patient’s occupation, what she does recreationally, and her iris color,” Dr. Gordon says.
A recent study found that presbyLASIK is a valuable option for presbyopic patients considering refractive surgery.5 In this study, 103 patients with an average age of 53.3 years underwent treatment with the VISX S4 system and follow-up from 1.1 to 3.9 years. Preoperative refraction ranged from -9.75 D to +2.75 D. Non-dominant eyes underwent peripheral presbyLASIK, and dominant eyes underwent monofocal refraction-based LASIK, wavefront-guided LASIK, limbal relaxing incisions or no treatment to optimize distance vision. At the last follow-up visit, 91.3 percent of all patients, 89 percent of hyperopes, and 92 percent of myopes reported complete spectacle independence, and 7.8 percent used glasses for less than one hour per week. Distance unaided visual acuity was at least 20/20 in 67.9 percent of hyperopes and in 70.7 percent of myopes.
“I’m not very enthusiastic about presbyLASIK in general. It cannot be undone, whereas inlays can be taken out,” Dr. Durrie says.
A recent study has found that Intracor safely and effectively treats presbyopia.6 The study was conducted in Croatia and included 95 eyes (49 patients had their non-dominant eyes treated and 23 patients underwent bilateral treatment). In this study, all eyes gained several lines of uncorrected near visual acuity and achieved good uncorrected distance visual acuity. A statistically significant improvement in both uncorrected near and distance visual acuity was noted at all visits.
Dr. Schallhorn notes that all of the technology that is currently available is a compromise. “Monovision is a compromise. We can provide good near vision in one eye, but that eye won’t have good distance vision, and the other eye will have good distance vision but not good near vision. And, accordingly, patient adaption is important. There is an optical compromise in providing essentially a multifocal effect. That applies also for excimer laser procedures. There is an element of compromise. The same thing goes for inlays. Some people are going to be more than willing to put up with that compromise. The watershed moment is when we can get away from this compromise,” Dr. Schallhorn adds. REVIEW
1. Yilmaz OF, Alagoz N, Pekel G, et al. Intracorneal inlay to correct presbyopia: Long-term results. J Cataract Refract Surg 2011;37:1275-1281.
2. Seyeddain O, Hohensinn M, Riha W, et al. Small-aperture corneal inlay for the correction of presbyopia: 3-year follow-up. J Cataract Refract Surg 2012;38:35-45.
3. Tomita M, Kanamori T, Waring GO 4th, et al. Simultaneous corneal inlay implantation and laser in situ keratomileusis for presbyopia in patients with hyperopia, myopia, or emmetropia: Six-month results. J Cataract Refract Surg 2012;38:495-506.
4. Alarcon A, Anera RG, Villa C, Jimenez del Barco L, Gutierrez R. Visual quality after monovision correction by laser in situ keratomileusis in presbyopic patients. J Cataract Refract Surg 2011;37:1629-1635.
5. Epstein RL, Gurgos MA. Presbyopia treatment by monocular peripheral presbyLASIK. J Refract Surg 2009;25:516-523.
6. Bohac M, Gabric N, Anticic M, Draca N, Dekaris I. First results of Intracor procedure in Croatia. Coll Antropol 2011;35 Suppl 2:161-166.