Many of the surgeons on our annual intraocular lens survey appear to be getting comfortable with presbyopic lenses, though there’s a fair percentage who aren’t ready to make the leap, citing possible qualitative vision issues or problems that could crop up if patients develop other ocular disease down the line. Toric lenses remain popular, however, and surgeons seem intrigued by the burgeoning technology of extended-depth-of-field IOLs.
These are some of the findings from this year’s e-mail survey on IOL preferences. This time around, 85 surgeons completed the questionnaire. To see how your approach and opinions stack up with theirs, read on.
Monofocal Lenses
Surgeons are looking for ease of use and the promise of crisp postop vision when they reach for a mono-focal IOL.
In this year’s survey, the Alcon Acrysof IQ monofocal was the option chosen by the largest percentage of respondents, at 50 percent. Twenty-eight percent say they use the Johnson & Johnson Vision Tecnis one-piece lens, and 6.4 percent each prefer the Bausch + Lomb enVista and Sofport, respectively.
A surgeon from Iowa says he uses the Acrysof IQ for most of his cases because of the “controlled insertion ... the lens tint reduces the complaints about white looking ‘too white and harsh.’ ” A surgeon from Texas says the Acrysof offers “ease of use and high-quality optics,” but notes that, “You must use a good technique for its implantation, as it must be well-centered.” An ophthalmologist from Illinois breaks it down this way: “Like: Pre-loaded; dislike: It’s not available in very high or low powers.” Another surgeon notes, “It’s stable, and gives predictable performance and ease of implantation.”
“I like the consistent centration and minimal PCO,” says Ridgewood, New Jersey, surgeon Douglas Liva. “I do not like the micro-glistenings that are less than in the past but still exist.”
 |
The Dalles, Oregon, surgeon John Willer, who prefers the Tecnis, says, “One, all J & J acrylic lenses share the same A-constant, so it only takes one place on my Lenstar for all lenses. Two, constant central thickness—it’s the same thickness regardless of power. Three: No inclusions!” A Texas surgeon agrees, saying that he likes the Tecnis’ “clarity, minimal posterior capsular opacification, ease of insertion through a small wound, lack of ‘reptile-eye pupil’ as opposed to the Alcon lens, and the cost.” Birmingham, Alabama, surgeon Robert Crain lists his likes and dislikes: “Like: It’s nearly glistening-free, has high negative spherical aberration and a rounded anterior edge,” he says. “Don’t like: the frosted edge.”
Matthew Fornefeld, MD, of Bloomington, Indiana, likes to use the B + L SofPort aspheric AO. “I like that you can put it in the sulcus if needed,” he says. “I don’t like the flimsy haptics; they can some- times get kinked traveling through the injector.” A Pennsylvania physician says he prefers the SofPort because of “no dysphotopsia, and it’s aspheric.” On the other side of the B+L coin, a surgeon who prefers the enVista says, “The aberration-free optic leads to fewer refractive complications.”
Presbyopic Lenses
In this year’s survey, surgeons provided the average number of implantations of each of the presbyopic IOLs on the market, as well as their average charge. Some surgeons selected more than one lens.
The most popular option, comprising 56 percent of the responses, is the Tecnis Symfony (non-toric) (average number implanted per month: 5; average charge/eye: $2,167). The AcrySof ReSTOR +2.5 was the next most popular choice, with 38 percent (average number implanted/month: 6; average charge/eye: $2,289). The Tecnis Symfony Toric was third, at 36 percent (average number/month: 4; average charge: $2,225). Twenty-four percent of respondents say they use the AcrySof ReSTOR Toric 2.5 (average number/month: 5; average charge/eye: $2,565).
A Tecnis Symfony user from Pennsylvania says he appreciates the depth of focus. “I’m getting excellent uncorrected distance vision (20/20 to 20/25) and good uncorrected near vision (J2) on almost all of the patients,” he says. “There are very few glare complaints and patients are very happy with the IOL in general.” A Symfony adherent from North Carolina agrees, saying, “There’s less halo, more toric rotational stability, better high add/near vision, [and I’m able to] expand to a wider range of ocular pathology (mild glaucoma, mild epiretinal membrane, mild age-related macular degeneration).”
 |
Alcon IQ ReSTOR 2.5 user Benjamin Mackey, MD, of Corbin, Kentucky, says that, with the ReSTOR, “Patients are mostly satisfied. Distance-vision quality is good and consistent. Near vision is usually good, but sometimes I have to use the 3.0 add for the second eye.” Dr. Liva has had a similar experience with the ReSTOR 2.5. “The reading could be better but would probably diminish the quality of the distance vision,” he says. “I prefer this lens due to its minimal side effects and excellent quality of distance vision. I am willing to sacrifice excellent reading vision to avoid the past problems of multi-focals such as ‘waxy’ vision and haloes at night.”
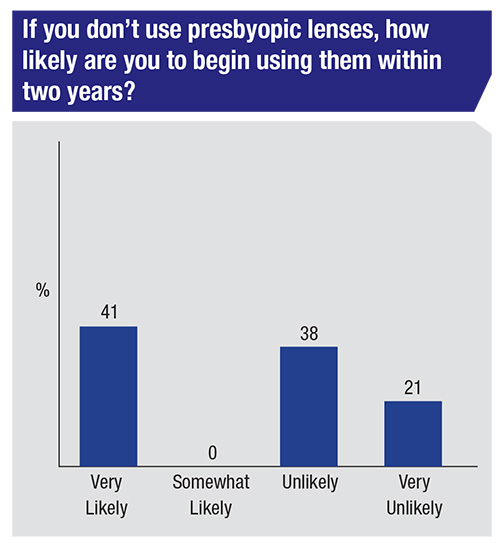
Looking down the road, 41 percent of the respondents who don’t currently use presbyopic lenses say they’re very likely to begin using them within two years. Fifty-nine percent of the physicians, though, say they’re either unlikely or very unlikely to start implanting these IOLs.
“The quality of vision is still not good enough with virtu- ally all of the presbyopic lenses,” avers a surgeon from Utah. “In addition, there are too many visual aberrations, glare, halo and dysphotopsias.” A physician from Arizona feels similarly, saying, “I’m not anxious to recommend a quality-of-vision compromise to my patients as well as long-term unknown consequences, such as [the lens’s use after the possible] subsequent development of AMD or mild lens movement over time.”
A surgeon from Florida, however, says he thinks he will try the Symfony. “It seems like it would have the best quality of vision, but also be a little more ‘forgiving’ of mild residual refractive error,” he says.
 |
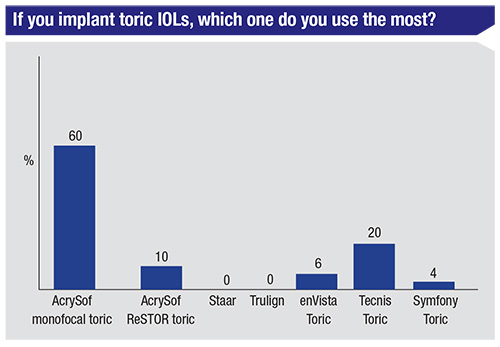
Toric Options
The AcrySof monofocal toric was the most popular toric lens on the survey, chosen by 60 percent of respondents. Next up was the Tecnis toric, at 20 percent. The new kid on the block, the recently approved enVista Toric, was chosen by 6 percent of the physicians.
A Utah surgeon who uses the AcrySof monofocal toric says he likes its “excellent visual quality and centration with minimum postop rotation.” Dr. Liva agrees, but says there’s more to consider than just the toric lens’s quality. “It has excellent stability,” he says. “The problem of torics is not the lens itself but the limited ability to measure the posterior corneal astigmatism accurately. Although new technology, such as the new Zeiss IOL- Master, has become available, the acquisition cost is difficult for a practice to justify. Considering that the reimbursement for laser biometry is decreased to just the level of the professional component for the second eye, a surgeon would have to do more than 100 scans just to pay the service contract on the device.”
An enVista user says he like the lens because, “Rotational stability is the most important to me. I use enVista and Trulign torics the most.”
One surgeon from Pennsylvania says there’s room for both the AcrySof and the Symfony on his shelf. “I use AcrySof and Tecnis a similar amount,” he declares. “I like the outcomes and the dependability of both of these IOLs.”