|
Here, I’d like to review the three categories of incisional IOP reduction and share a simple mnemonic device that you may find beneficial when deciding on a procedure.
Three Surgical Pathways
Once you’ve concluded that an incisional approach is necessary to lower IOP—assuming you’ve decided cataract surgery alone is not the best way to go for your patient—there are three alternatives you could choose: You can create a new drainage system; improve the existing drainage system; or decrease aqueous production. The first and most commonly chosen option is creating a new drainage system for the eye, which you can do by creating a filter (with various options) or inserting a glaucoma drainage implant. When you choose to create a new, alternative drainage system, you are essentially giving up on the patient’s own natural drainage system—although many surgeons may not think of it this way. In fact, the patient’s own natural drainage system atrophies further when you successfully direct aqueous humor away from it.1
Filtration surgery is consistently the most potent option for IOP reduction, but it comes with the most risk, including unpredictable wound healing. These risks are worth taking when a patient has advanced disease and needs a low pressure. However, many patients with mild to moderate glaucomatous damage don’t need subnormal pressures.
|
The third approach to lowering pressure is to decrease aqueous production via ciliary body ablation using an option such as endoscopic cyclophotocoagulation. All three approaches—creating a new drainage system, enhancing the one that’s there, or reducing aqueous production—have pros and cons that make each type of surgery more appropriate in specific patient situations.
An Alphabetical Checklist
Knowing that you have those options, how do you decide which one makes the most sense when incisional surgery is the most appropriate way to proceed? A simple mnemonic device using the first five letters of the alphabet may help, especially in the early stages of deciding what is best for your patient.
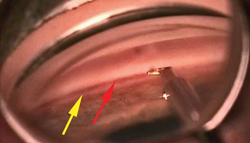
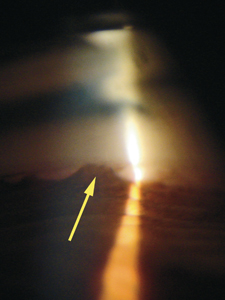
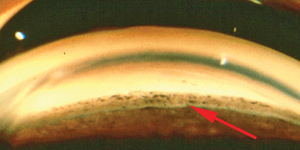
“A” stands for two factors: angle and age. The appearance of the angle is important because it reveals whether or not you have the option of salvaging the patient’s own collector system using one of the minimally invasive surgeries. The key here is mild to moderate disc damage and an open angle with good landmarks.
Obviously, if you decide to go in this direction, gonioscopy is critical in order to visualize the angle structures. For example, if gonioscopy reveals peripheral anterior synechiae, or a poorly seen scleral spur or a sclerotic meshwork, enhancement of the patient’s natural collector system is unlikely to be effective. Most importantly, if you can’t find the scleral spur, that means the angle structures are confusing, and that’s not a good sign for minimally invasive surgery (See example, above). In short, if you can’t see clearly what’s happening in the angle, that should make you lean more toward creating a new drainage system for the patient.
|
“A” also stands for age, which refers to both the age of the patient and the “age” of the disease. Patients with early glaucoma and fewer years of glaucoma drop therapy may have a better chance of enhancing their distal collector system. Someone who is 80 years old and has been on drops for 50 years is likely to have a collector system that’s in bad shape. It’s not likely you’ll have luck rejuvenating that. (However, that may change as we determine what medications are best to inject into the collector system at the time of surgery to enhance outflow.)
So, angle and age are somewhat interconnected. If a patient is fairly young, hasn’t been on drops for too long and you can see the meshwork clearly, trying to salvage the patient’s own natural collector system to enhance outflow may be a very reasonable way to proceed. At this time, minimally invasive glaucoma surgery using the Trabectome or the iStent is worth considering because the conjunctiva is not violated. You can explain to the patient that you’re trying to improve his own natural drainage system, but if this fails, more aggressive procedures are still available and have not been compromised.
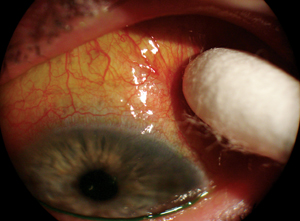
“B” stands for blood-aqueous barrier. If a patient has inflammatory or neovascular glaucoma and the blood-aqueous barrier is very disturbed, that should push you in the direction of creating a new drainage system for the patient—typically a glaucoma drainage implant tube shunt. If the blood-aqueous barrier is not functioning normally and there’s a lot of inflammation, you’re not likely to get the patient’s own drainage system to work, because PAS will reform and shutdown the collectors.
|
“D” is for disc and discussion. If the patient has a very sick disc as a result of very advanced glaucoma and needs a very low pressure, you’ll have to lean more toward the risk associated with trabeculectomy (or the similar ExPRESS procedure), because trabeculectomy consistently produces low pressures. If the patient is rapidly going blind from very advanced disease, it’s worth the risk. On the other hand, a lot of patients’ optic discs have mild to moderate disease, and they don’t initially need a pressure of 10 or 12 mmHg. That’s an ideal situation in which to examine the angle and ask whether you can improve the natural drainage system. Either way, the condition of the disc helps you decide which direction to go.
As already noted, one big advantage of trying minimally invasive surgery on a patient with a mild or moderately damaged disc is that if the pressure doesn’t drop as much as you’d like, you haven’t limited your future options; you haven’t touched the real estate where you’d do a trabeculectomy. Of course, some surgeons would prefer to use the procedure most likely to produce a big initial drop in pressure as their first option, and many doctors simply stick with what they know works—typically, trabeculectomy. That’s a perfectly reasonable choice, but trabeculectomy involves far more risk than the minimally invasive procedures, and that’s a good argument for not automatically choosing it.
“D” also stands for discussion with the patient. In fact, the patient might be happy to know that you’re trying the lower-risk option first. Certainly, when risk is involved, the patient deserves a say in which option is chosen. However, most patients take their lead from the doctor, so their choice will be heavily influenced by the way you present the options. If you say, “We have this other procedure that’s minimally invasive, but it doesn’t lower the pressure as well, so I don’t recommend it,” the discussion is over.
As long as you feel comfortable offering a minimally invasive option, it’s important to present the option in an unbiased way, listing the pros as well as the cons. For example, you could say: “We have an alternate procedure that may not lower the pressure quite as much, and you still may need to use a drop afterwards, but the risks associated with it are considerably less, and it involves less postop healing and follow-up. If it turns out that we still need to lower the pressure further, the other options will still be open to us.” For some patients, that’s a worthwhile trade-off.
“E” is for expertise. When deciding which surgical option to choose, you have to know the patient, but you also need to know your limits. If you’re offering the minimally invasive surgical options, in addition to maintaining your procedure-specific surgical skills, you’ll need to maintain your gonioscopy skills; angle anatomy is a crucial part of this decision-making process. If you don’t feel that your proficiency is at the level it needs to be, it may be worth reviewing some gonioscopy chapters. Then, gonioscope every eye you can in the clinic, just so you can start to appreciate the normal variations you’re likely to encounter.
The bottom line is that your level of expertise in these surgeries—and in gonioscopy—should have some influence on which of the available surgical options you choose.
Lowering Aqueous Production
The third category of glaucoma surgery, lowering aqueous production, tends to be underutilized. I believe the primary reason for this is that in the past most surgeons equated cyclodestruction with lowering pressure in blind eyes. However, modern day cyclodestruction, including endoscopic cyclophotocoagulation, is a safe and effective procedure, as numerous studies in the literature have documented. It’s another minimally invasive option that can be a valuable surgical alternative in many situations.
In terms of going down the ABCDE list, you might choose to lower aqueous production if the angle looks confusing to you, because that might indicate that increasing the outflow would be problematic. I most commonly perform ECP with cataract surgery, because the patient should be pseudophakic in order to laser the ciliary body. Age might also be a factor. Suppose your patient is elderly, a little frail, is taking a blood thinner and has a pressure of 30 mmHg. You don’t want to stop the blood thinner and you don’t want the patient on the operating room table for long. You don’t want to create a filter because you’re afraid of a suprachoroidal hemorrhage or a catastrophic event. You may say to yourself, “This patient’s a perfect candidate for a cyclo-destructive procedure, because it doesn’t take long to do, it’s minimally invasive and I won’t have to worry that the patient may bend, stoop or strain postop.” In this situation I’d probably do an ECP or even a transscleral cyclophotocoagulation.
Getting the Big Picture
Of course, when choosing a surgery, everything is interrelated. If you use the ABCDE system, it’s not so much that one letter will tell you how to proceed; it’s more that the overview you get by going down the list will help clarify the factors you need to consider. Then, if you know your patient and your skill level, you’ll make the optimum surgical choice. REVIEW
Dr. Fellman is a clinical associate professor emeritus at the University of Texas Southwestern Medical Center in Dallas, and president of Glaucoma Associates of Texas.
1. Johnson DH, Matsumoto Y. Schlemm’s Canal Becomes Smaller After Successful Filtration Surgery. Arch Ophthalmol 2000;118:9:1251-1256.



