At the 2008 meeting of the American Society of Cataract and Refractive Surgery, AMO announced an upgrade for the venerable IntraLase FS femtosecond laser that greatly increases its treatment speed, as well as adds a couple of other features. Here's a look at what's been changed on the device and the possible clinical benefits of the new upgrade, called the iFS.
150-Khz Repetition Rate
Surgeons who liked the benefits of the 60-Khz IntraLase laser upgrade will probably be pleased to learn that the company has upped the machine's speed to 150-KHz on the iFS.
"With a rate of 150 KHz, the surgeon has a choice," says Perry Binder, MD, who is a consultant for AMO. "First, he can choose to finish the operation quicker. To do this, he uses the same energy and spot/line separation settings on the laser that he used with the 60-KHz system and can create a 9-mm flap in eight to 10 seconds, compared to 17 to 20 with the 60-KHz FS. The advantages of this are less discomfort for the patient, less subconjunctival hemorrhage, less suction time on the eye and a faster patient throughput.
"Or, the surgeon might want to make the flap-lift step smoother and easier. If that's the case, he can place the spots closer together, which allows him to reduce the energy delivered to the eye. This can mean less inflammation and less of a chance of postop transient light sensitivity. Also, with less energy and smaller spot separation, you decrease the size and density of the opaque bubble layer."
Arturo Chayet, MD, Review's refractive surgery editor, performed the first 200 cases using the new system and chose the conservative approach to setting his machine. "We chose conservative parameters of a 0.6-µJ energy and a spot/line separation of 6 µm/6 µm," he says. "With that, the average time to make a flap was 14 seconds. In comparison, the 60-KHz laser using an energy of 0.8 µJ and a spot/line separation of 8 µm/8 µm would take 24 seconds. These corneas have been very quiet from day one, and we haven't seen a single case of photophobia during follow-ups as long as three months." He says this is in contrast to cases in which the surgeon might use a little higher energy, which, in the past, has occasionally resulted in some photophobia at around the three-month postop point.
"The amount of OBL has been minimal—not zero—but minimal," Dr. Chayet adds. "The clarity and quality of the bed is better than it was with the 60-KHz laser. This allows the surgeon to use the excimer without having problems with the eye tracker."
A New Angle on Flaps
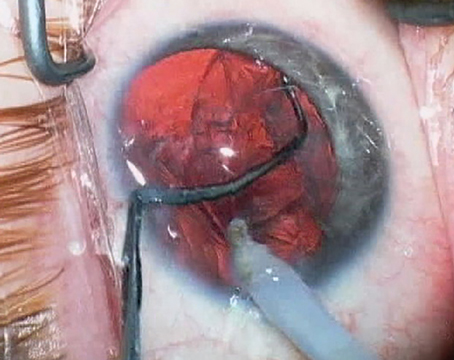
The iFS system also allows the surgeon to increase the angle of the flap's side cut to 150 degrees, a configuration that the company calls an inverted bevel. With this type of angle on the side cut, when viewed in cross-section the flap notches in below a triangular lip of cornea that the company hopes increases the strength of the flap when it's laid back into place. This is in contrast to the 70- or 90-degree side cuts, in which the flap is seated in a way similar to a manhole cover.
In an unpublished study in rabbit eyes performed by AMO consultant Michael Knorz, MD, of Mannheim, Germany, Dr. Knorz made flaps with a microkeratome, an iFS using a 70-degree side cut and the iFS using a 140-degree side cut. After letting the cuts heal, he glued contact lenses to the corneas and then tried to lift the flap/contact lens, using a force gauge to measure how difficult it was. The microkeratome flaps required 210 g of force to lift, the 70-degree side cut flaps needed 492 g and the 140-degree flaps required the most force, 687 g.
Dr. Chayet also took a look at flaps with the inverted bevel in 30 patients. For each patient, in a random fashion, he created a flap with a 70-degree side cut in one eye and one with the 150-degree cut in the fellow eye. He then laid the flaps back down. About a month later, with no knowledge of which eye had received which particular kind of side cut, he tried to lift the flaps to do the refractive ablation, noting the difficulty with which the flaps came up. In 64 percent of the cases, he noted more resistance when trying to lift the 150-degree flaps.
"Because of the angle, there may be more fibrosis, making the connection stronger," says Dr. Chayet. "So, there's the potential for a stronger flap." This may be a double-edged sword later on, however, if the patient requires a re-lift enhancement. "It will be a little bit harder to lift it for an enhancement," Dr. Chayet acknowledges. "Not so much the interface, but the flap edge."
A New Shape
The third alteration AMO made to the laser is the option of making oval, elliptical flaps. The maximum ovality allowed by the system is 12 percent.
Dr. Binder says that one benefit of the elliptical flap is that it severs fewer corneal fibers than a circular flap, since it's narrower in one dimension. He says this may mean less biomechanical weakening of the cornea. It may also be helpful in cases in which the ablation will hit the hinge of a circular flap. "In this situation, with a circular flap, you could change the hinge angle and push it farther out," says Dr. Binder. "But then you have a smaller hinge angle so the flap's not as stable. Your other option might be to use an elliptical flap with a temporal hinge. This lets you push the hinge out but still keep the larger hinge angle. You can do the ablation but the flap is still stable."
The iFS system still requires U.S. Food and Drug Administration 510(k) clearance before AMO can market it. The company expects the clearance in late spring of 2008. AMO says both 60-KHz systems and older units could be upgraded, though it hasn't established a price for the upgrade yet.