As many surgeons know, making patients happy with their premium intraocular lenses can be a challenge. It only gets harder when the premium lens is relatively new to the market and has a unique design. Though the PanOptix trifocal IOL (Alcon) offers the potential benefit of providing sharp vision at distance, intermediate and near, surgeons may still have questions regarding patient selection and what kind of results to expect with the lens. Here, experts share their insights on the new IOL.
The Lens’s Design
The PanOptix is composed of foldable acrylic, and has a 6-mm optic. The optic diffractive structure is in the central 4.5-mm portion of the optic and divides the incoming light to create a +2.17 D intermediate and a +3.25 D near add power at the IOL plane (approximately +1.65 D and +2.35 D at the corneal plane).1 The anterior surface is designed with negative spherical aberration.
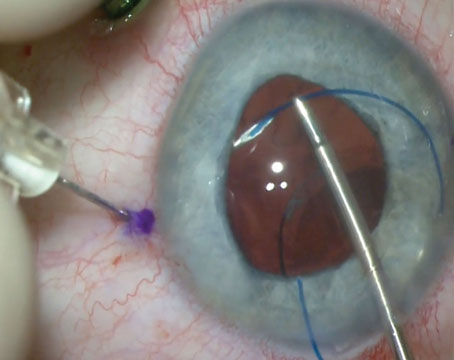
The posterior surface of the toric PanOptix is marked with six indentations on the flatter meridian.
Where Trifocals Fit in the OR
Surgeons note that there are some noticeable differences between trifocals and other multifocal lenses that use a bifocal approach. “[Bifocal multifocals] have a specific near point,” explains South Carolina surgeon and Alcon consultant, Kerry Solomon. “Depending on the add of the lens—there’s a +2.25, +2.75, +3.0, +3.25, and a +4 add, for example—there’s one specific point in space where things are clearest with a little bit of a range. The trifocal has two focal points, and they’re spaced out such that there’s very little drop-off between the focal points. A multifocal, for example, with a +3 add falls off at intermediate vision. A multifocal with a +1.5 add, or an extended-depth-of-focus lens with a +1.5 to +1.75 add falls off in the near. A trifocal, because it has more than one area of best focus, gives a larger range of vision.”
Though trifocal proponents say they appreciate the lenses’ range of vision, many use them as just one of the arrows in their quiver. Having both trifocal and EDOF lenses gives the surgeon more options for patients, according to Uday Devgan, MD, who is in practice in Los Angeles. “EDOF lenses like the Symfony (Johnson & Johnson Vision), which have diffractive rings, seem to function like a low-add bifocal diffractive IOL with reasonable intermediate and far vision, but not quite enough near vision without spectacles,” he says. “The Vivity EDOF from Alcon, which is already available in Canada, does not have diffractive rings on it, but instead is a newer type of of EDOF lens that uses other optical methods to elongate the focal range to a degree.”
If you’re planning to get involved with the PanOptix trifocal lens, surgeons say to expect certain advantages and disadvantages. “The idea of EDOF IOLs having a single wide peak in the defocus curve, versus multiple peaks, does provide a degree of forgiveness when it comes to refractive targeting,” says Daniel Chang, MD, a Johnson & Johnson Vision consultant who practices in Bakersfield, California. “We’d all like outcomes with perfect distance, intermediate and near vision, but surgeons unfortunately miss the refractive target or leave residual astigmatism more often than we like to admit.
 |
“When this happens, we’re shifting the defocus curve either to the right or to the left, so the distance peak doesn’t hit plano,” he continues. “If we have a broader peak and we miss the refractive target, we can still maintain good distance vision, albeit at the possible loss of near. In comparison, with bifocal/trifocal IOLs, the distance peak is going to get smaller, so it’s more critical to nail the refractive targets. From a usability standpoint, EDOF technology offers better refractive forgiveness than bifocal/trifocal IOLs. Additionally, since EDOF IOLs like the Symfony provide image quality that’s comparable to aspheric monofocals, common issues like missing the refractive target, posterior capsule opacification and dry eye can be better tolerated because of the superior image quality.”
He adds that he doesn’t intend to use the PanOptix, because of concerns about the AcrySof platform. “While I think trifocal IOLs can have a benefit, I have concerns about PanOptix both from a material and from an optical properties standpoint,” he says. “The high-index AcrySof material has high reflectance, glistenings and poor chromatic aberration, which can lead to image-quality issues. It can also have frost along the edges, is prone to scratches during folding and implantation, and tends to pit more easily from YAG capsulotomies than other hydrophobic acrylic materials.”
However, Boston’s Bonnie An Henderson, MD, who consults for Alcon, believes that trifocal lenses are a valuable addition to the currently available IOLs. “No lens is perfect, but trifocal lenses deliver what they promise, which is near spectacle-independence,” she says. “Because the previous multifocal IOLs were bifocal lenses, they only provided uncorrected vision at two distances rather than three. The launch of trifocal IOLs has been a welcome addition to the presbyopia-correcting IOL armamentarium. Originally, I was concerned that a trifocal IOL would increase the risk of positive dysphotopsias. I have been pleasantly surprised that this hasn’t been the case. In fact, the trifocal IOLs have been well received by patients without an increase in the incidence of unwanted side effects.”
According to Dr. Solomon, the secrets to success with trifocals are patient selection, good surgical planning in order to make sure you hit the refractive target, and patient education on the front end. “Let patients know about the night-vision issues so they’re not surprised,” he says. “And make them aware that, even with a good surgical plan that’s striving to hit the target refraction, there’s a 15- to 20-percent chance that you’ll need to do a secondary procedure like a PRK or LASIK touch-up, to get them where they need to be, and that’s expected. However, if you have a good, healthy eye, hit the target refraction and perform good patient selection, you should have terrific results and very happy patients.”
Patient Selection
According to Dr. Solomon, anyone with healthy eyes, including a healthy ocular surface, is a candidate for trifocal lenses. “I’ve also had good success using them post-refractive surgery,” he says.
He also adds that it’s important for patients to be told that the lens splits light. Because the lens has rings in its design, patients will notice rings and halos at night. “In the FDA studies, the vast majority of patients, 95 percent, found these to be very mild or moderate, tolerable, and not a distraction at all,” Dr. Solomon says. “Five percent of the patients rated the night vision issues as severe. However, even in that 5 percent, the majority didn’t want the lens removed because the rest of their vision was so good that they tolerated the night-vision issues. I reassure patients that the rings are supposed to be there. I show them an image of what the rings look like, and the vast majority of patients say that seems fine or that they’re already experiencing that with their cataract. I explain that it will look different after the cataract removal, but it shouldn’t be distracting to them. The vast majority of patients have no issues, and the overwhelming majority, once they’re implanted, do very well. Approximately a third of my patients don’t notice the rings even though we know they’re there; one-third of them notice them but say they get better with time—they don’t, but the brain adapts; and one-third say they notice the rings to varying degrees but they don’t limit their vision. In the rare instance that this does limit their vision, we can take the lens out and exchange it for something else.”
It’s important to have this conversation with every patient, because some people don’t want even a small chance of compromised night vision, surgeons say, adding that this might be a niche to be filled by an EDOF lens like the Symfony or Vivity.
Also, patient expectations need to be managed, says Dr. Devgan. “There is no such thing as the fountain of youth for vision,” he says. “Even with a trifocal, you’re not going to see like a 25-year-old. With trifocal lenses, you still have the compromises of splitting the light, which is what gives you nighttime glare and halo, as well as decreased contrast. I ask my patients to choose between two sentences: (1) ‘I want the very best quality of vision, the best night vision, the best contrast, and I will wear reading glasses,’ or (2) ‘I don’t want to wear reading glasses and, to achieve that, I’ll happily sacrifice some quality of vision, especially at night when I’ll see some glare and halos.’ Usually, with one of those sentences, I can tell whether a patient has the right mental attitude for the lens. If patients say they want perfect quality of vision, and they also don’t want to wear reading glasses, then we simply don’t have anything that will meet their expectations.”
Surgical Planning
Surgeons say there are a couple of considerations when you intend to implant a trifocal lens.
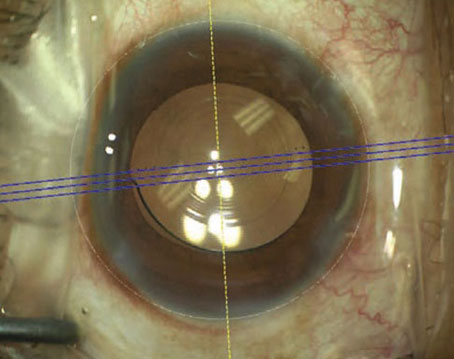
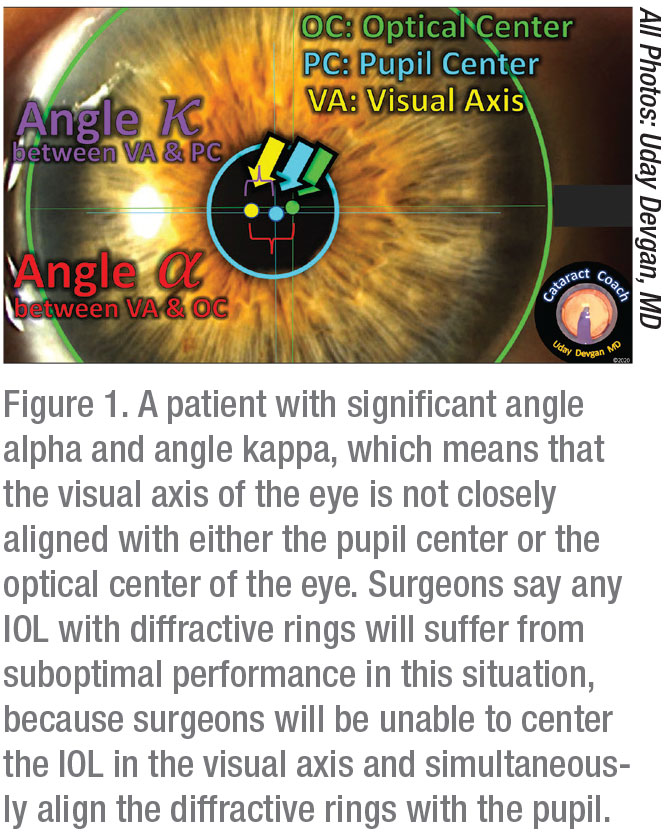
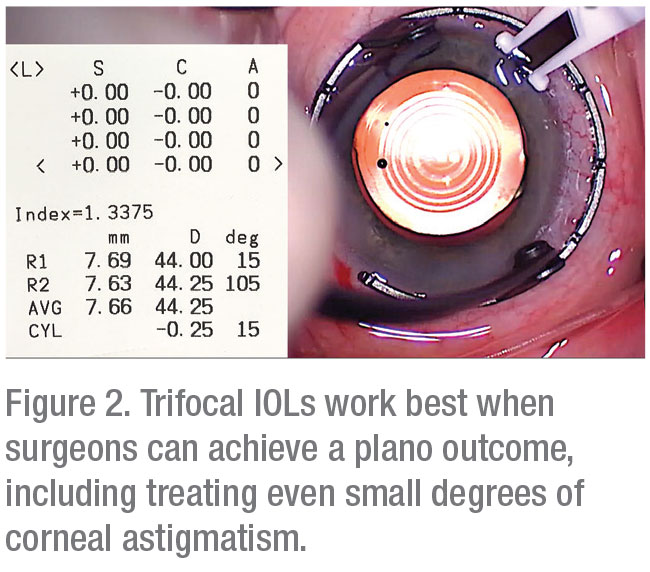
“You should have an otherwise completely healthy eye,” Dr. Devgan avers. “Any problem that exists in the eye tends to be magnified when you put in a light-splitting lens. These lenses are for completely normal eyes in which you as the surgeon can hit your refractive target, even treating small degrees of astigmatism to achieve a plano outcome. I also preoperatively check the angle alpha and angle kappa to see how well the pupil is lining up with the visual axis. During surgery, you’re going to place this diffractive lens in the center of the pupil. If their visual axis is somehow off, they may not achieve good-quality vision.” To help with the implantation of the toric version of the lens, Alcon offers a web-based calculator at https://www.myalcon-toriccalc.com/.
 |
In terms of results, in the U.S. Food and Drug Administration study of the lens, half of the 127 PanOptix patients could see 20/20 at near binocularly, uncorrected, vs. just 0.9 percent of the monofocal IOL patients (total n=111). Ninety-two percent could see 20/25 or better at near vs. 9 percent of the monofocal patients. At intermediate distances, 73 percent of the trifocal patients could see 20/20 vs. 22.5 percent of the monofocal group, and 93.7 percent of the trifocal patients could see 20/25 or better compared to half of the monofocals. (Monofocal IOLs gave slightly better uncorrected distance vision in the study, with 78.4 percent of monofocal patients seeing 20/20 or better vs. 73.2 percent of the trifocal patients; and 94.6 percent of the monofocal group seeing 20/25 or better, compared to 92 percent of the PanOptix group.1)
Starbursts, halos, and glare were the most frequently cited visual symptoms in the PanOptix group. For glare, 3.2 percent rated it as “severe,” vs. 1.8 percent of the monofocal patients in the study. In terms of halos, 12.6 percent of the PanOptix patients described them as “severe,” compared to only 0.9 percent of the monofocal patients. Finally, 16 percent of the PanOptix patients said their starbursts were “severe,” vs. 1.8 percent of the monofocal patients.1
When implanting premium lenses, Dr. Chang says that the surgeon has to strike a balance between image quality, range of vision and night-vision symptoms. “With both refractive and diffractive optics, the more range of vision that you provide, the more image quality you stand to lose,” he says. “Unless you compensate for your range-of-vision increase with something like the correction of chromatic aberration, visual quality can suffer. From a night-vision standpoint, more near vision results in more off-axis light that can lead to dysphotopsias, such as glare, halos and starbursts. So, the reason the Crystalens or the ReSTOR 2.5 has minimal night vision symptoms is because they provide minimal near vision. The relationship isn’t hard-and-fast, but the trend is tied to the optics.” REVIEW
Dr. Chang is a consultant with Johnson & Johnson Vision, and he is an investigator for the IC8 IOL for AcuFocus. Dr. Devgan was formerly a consultant for Alcon, AMO/Abbott and Bausch and Lomb. Drs. Solomon and Henderson are consultants for Alcon.
1. FDA Summary of Safety and Effectiveness Data, Alcon PanOptix. https://www.accessdata.fda.gov/cdrh_docs/pdf4/P040020S087B.pdf. Accessed September 22, 2020.