A perfectly round, continuous curvilinear capsulorhexis sets the tone for the rest of a cataract surgery case, and is arguably the hardest part to learn. The feel of the capsule during cutting has been likened to easily-torn cellophane,1 so it’s understandably hard to consistently create a perfectly round rhexis that will cover the lens for 360 degrees. It’s well worthwhile though, because such a circle will support your IOL and keep it well positioned. The advent of femtosecond-created capsulotomy contributed to the creation of predictably sized, quick and reproducible capsulotomies, but at a significant extra cost not reimbursed by insurers. Here, surgeons discuss two devices currently available in the United States and two emerging technologies that aid in creating perfect capsulotomies without a femtosecond laser.
Zepto
Vance Thompson, MD, of Thompson Vision in Sioux Falls, South Dakota, remains a femtosecond laser enthusiast, but finds that Zepto (Mynosys; Fremont, California) is a valued addition to his cataract-surgery armamentarium. “It’s become mainstream in my practice; it’s not just a research tool anymore,” he says. “I’m a big fan of femto. I have a femto. But for surgeons who may not want to invest in femto, but like the idea of an automated capsulotomy, I think Zepto is a great answer.”
The Zepto, FDA approved in 2017 and commercially available, consists of a small console that provides energy to a disposable handpiece equipped with a flexible nitinol ring. The Zepto ring folds to go through a small incision, typically 2.4 mm, then springs back into circular shape inside the eye. To ensure 360-degree contact with the anterior capsule, the Zepto employs a clear silicone suction cup over the membrane to gently draw it towards the ring. A quick 0.4-msec pulse of thermoelectric energy instantly creates a round capsulotomy about 5.2 mm in diameter. The surgeon then retracts the cutting element and withdraws it through the wound and the surgery proceeds.
Dr. Thompson likes the Zepto for both premium IOLs and difficult cases, such as intumescent milky cataracts. “In people with corneal scarring, whether it’s from RK or previous trauma, it can be difficult to use femto, and the Zepto can be very helpful. In small pupils you can’t do femto and it’s a challenge to do manual, but you can fit the Zepto technology inside a small pupil and get a nice capsulotomy,” he says. “People have also found it valuable in pediatric cases, which pose some of the most challenging capsulotomies: Being able to just do it all at once with the Zepto has really been helpful for pediatric cataract surgeons. It’s been a useful device for challenging situations.”
Dr. Thompson uses the Zepto for all of his premium cases because he can align it by viewing the Purkinje reflexes through its clear silicone suction cup. “I love the Purkinje method of centering the capsulotomy,” he says. He adds that using OCT to center femtosecond-created capsulotomies has demonstrated that individual visual axes are not always at the center of the pupil. “People’s pupils are oftentimes nasal or temporal or superior or inferior,” he says. “They vary in their location with respect to the lens. And so with OCT-guided femtosecond lasers, my rate of 360-degree capsular overlap went way up compared to manual and to a pupil-centered femtosecond laser. But one of the problems with OCT guidance was that the tilt control was sometimes not as good as it could be. Sometimes, patients had a little more tilt and the tilt compensation didn’t always allow for that overlap.
“Then Daniel Chang and George Waring published an article2 on using the subject-fixated coaxial light reflex, which is the Purkinje image with the patient fixating on the microscope light to center the capsulotomy,” Dr. Thompson continues. “So when Zepto entered the arena, it kind of reminded me of a cookie cutter: Zepto is a perfectly round device that I can land right on the capsule and center on that first Purkinje image with the patient fixating. It became an even more consistent way to achieve a full 360 degrees of capsular overlap. And it fits right into my OR. It isn’t like I need to stop to add a femtosecond laser outside the room because it fits right on the surgical set.”
Dr. Thompson says the Zepto is easy to use, but he has a few pearls for getting optimal outcomes with it. “One of the nice things about the Zepto is that it sucks right onto the capsule and creates the capsular opening for 360 degrees all at once. It’s important to achieve consistent suction on the capsule for 360 degrees so that the nitinol ring is in close approximation to the capsule. I’m now over 900 capsulotomies in with Zepto, and I’ve had free-floating capsulotomies every time, but I have had three anterior capsule tears that I’ve needed to manage. None of them extended posteriorly; and they all happened in high myopes,” he says. “What I noticed was that with deep anterior chambers, if I didn’t have good approximation for 360 degrees of the nitinol ring, the area that was a little farther from the capsule would make a weaker capsulotomy.” He recommends taking the manufacturer’s training and working with surgeons who have a lot of experience with the device. “When the flange, or suction cup, is splayed out nicely for 360 degrees, that nitinol ring is in great approximation with the capsule. If that flange is only splayed out for 300 degrees, for example, so that for 60 degrees it’s more vertical and not splayed out, the nitinol ring isn’t as close to the capsule as it should be in that area. When that occurs, the surgeon shouldn’t deliver the energy. It’s important to follow the procedures that are taught in the surgeon Zepto training, and to be comfortable with the idea that if you don’t have perfect centration, or if you don’t have 360 degrees of the flange splayed out beautifully with suction, then you can turn suction off and not deliver the energy: You can then re-approximate it, re-engage suction and you’ll often get it exactly the way you want so that you can go ahead and deliver the energy. Or, if you can’t get it approximated the way you want it, you have the choice to disengage suction and just do a manual capsulotomy like you’re trained to do,” he says.
In addition to reducing surgical costs compared to femto, Dr. Thompson says that Zepto-created capsulotomies appear to be strong, relative to those created via femto and manual methods.3 “It cuts the collagen, and, since it uses heat, it creates an upturn of the collagen fibers, which is also what creates its strength,” he explains.
“My ultimate goal in cataract surgery is to center the capsulotomy on the center of the lens so that the patient has 360 degrees of anterior capsule overlap of the optic. Then, when capsule contraction happens like it does in everyone, the lens will be stable and not decenter or tilt. This is how we achieve long-term quality vision after cataract surgery, and Zepto has allowed me to achieve this overlap with more consistency than any other technology or technique I have used previously,” says Dr. Thompson.
Verus
Another femto alternative for the creation of a continuous curvilinear capsulorhexis is markedly lower-tech than the other devices described here: The Verus ophthalmic caliper (Iantech; Reno, Nevada) is a singe-use silicone ring guide with an internal diameter of either 5 or 5.5 mm, etched with micro-patterning on the top and the underside to prevent it from moving laterally during capsulorhexis. It flexes to enter the eye through a 2.4-mm incision after the surgeon fills the chamber with dispersive OVD.
Michael Taravella, MD, professor of ophthalmology at the University of Colorado School of Medicine, was an early adopter of the device as his colleague, Malik Kahook, MD, developed it. Dr. Taravella finds the Verus a helpful adjunct to the femtosecond laser in certain cases. “I’ve come to believe as a cataract surgeon that the rhexis is probably the most important step in cataract surgery because even though it’s rare to have a posterior capsular tear, if you do have one you have many options in terms of lens positions if the rhexis is good. If you have a well-centered rhexis and it’s properly sized, you can handle a case in which a complication occurs because you’ll have an alternate place to put the lens. For example, you could put the haptics of a three-piece IOL in the sulcus and do optic capture, and that eye will turn out great. You could even do that with a three-piece multifocal lens if you had to. If you don’t have a femto and you really want a well-centered rhexis, the Verus gives you some choices when trying to create a perfect circle,” he says. Dr. Taravella says he finds the Verus useful in settings where a femtosecond laser isn’t available, as well as in those cases where using one isn’t feasible. “There are certain situations where I think it’s helpful. I’ve done more than 10,000 cases, so obviously, I don’t feel like I need it for help in learning the capsulorhexis. But I think if you’re really trying to get a well-centered, good rhexis in a premium IOL case for a toric or multifocal lens, it’s nice to have—especially if you don’t have a femtosecond laser available. You can get a nice, circular, well-centered rhexis, which I think helps in terms of estimated lens position and just the overall result and the way the lens looks in the eye,” he says.
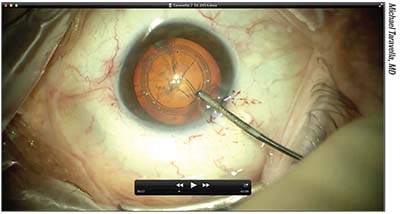 |
| Video capture of Dr. Taravella making a capsulorhexis with the Verus, a single-use silicone ring caliper. Micro-patterning on both sides of the ring acts as a lateral brake to keep the rhexis from extending radially. |
There are some eyes that aren’t good candidates for femtosecond capsulotomy, even when it’s available. Verus may be a handy, low-cost alternative in these select cases. “Sometimes you have a cornea that’s a little too steep or too flat and you can’t dock,” says Dr. Taravella. Complex cases like hypermature white intumescent cataracts are another example. “You can put the Verus ring down on top of the capsule, and it does help prevent an Argentinian flag syndrome. I think this a good device to help prevent the rhexis from going radially in some situations.”
As an experienced surgeon and mentor, Dr. Taravella appreciates the Verus as a guide to help newer practitioners building their CCC skills. “I work with residents and fellows,” he says, “and I think that especially with residents early on, it’s a useful teaching guide. I do think it has some applicability to residents learning how to do a rhexis.”
A small restrospective controlled case series comparing Verus-assisted with freehand CCC suggested that the Verus is effective in improving the rate of circular, centered CCCs at the targeted size, while adding a trivial amount of extra time to the procedure.4 Another open-ring-shaped guide, the ORGC (Lucid Co.; Seoul, South Korea) produced similar results when compared to freehand CCC.7
Dr. Taravella notes that for all its ease of use, however, the Verus does have a slight learning curve that the surgeon must surmount. “You fill the eye with dispersive viscoelastic, put the ring in, and then tamp it down. The Verus has to be in very good contact with the capsule before you start your rhexis,” he stresses. “Other than that, you just proceed as normal. But as you create your tear, you lay the edge of your rhexis right against the edge of the ring, like a piece of paper against a ruler. When I first used it, I tended to use it as a guide, and my rhexis was a little smaller than I had planned. Then I learned to sort of lay the capsule against the edge of the ring, almost like you’re tearing a sheet of paper against a ruler. That works pretty well. I haven’t seen any radial extension with it in my hands.
“The nice thing about it is that it’s fairly straightforward, easy to use and a lot less expensive than a femtosecond laser,” continues Dr. Taravella, who acknowledges that he uses the Verus relatively infrequently. “Normally I can get a good dock, and I love using the femtosecond laser because a lot of times I’m also doing other things like trying to correct astigmatism with it,” he says.
CAPSULaser
One alternative to the femtosecond laser for capsulotomy currently unavailable for clinical use in the United States is the CAPSULaser (Excel-Lens; Livermore, California), a small continuously firing orange laser that attaches underneath the surgeon’s microscope, and works with a shoebox-sized console that will fit easily into the OR. The CAPSULaser aims to incorporate the capsulotomy benefits of a femtosecond laser without necessitating a dedicated laser room in the surgical suite, with lower cost to own and operate.
Unlike some other femto alternatives, the CAPSULaser isn’t pulsed; it fires continuously to cut in a circular pattern, creating a tag-free capsulotomy in one second, according to the manufacturer. For the capsule to absorb the CAPSULaser’s cutting energy, the surgeon must stain it with trypan blue, and then wash it out. (Excel-Lens offers proprietary blue intraocular dye and cohesive and dispersive OVDs, which are CE-certified.) The patient fixates on a beam of light while the surgeon places a handheld contact lens over the eye to aim the beam, which is controlled by a foot pedal. The device can cut a capsulorhexis in diameters ranging from 4.5 to 6 mm in 0.1-mm increments. The CAPSULaser’s energy transforms the collagen of the rhexis edge, making it smooth and elastic, according to the manufacturer.
Richard Packard, MD, FRCS, FRCOphth, presented clinical trial data at the recent American-European Congress of Ophthalmic Surgery’s European Summer Symposium in Berlin. In 125 patients randomized to CAPSULaser or manual capsulorhexis, Dr. Packard reported that the CAPSULaser produced greater circularity and centration and achieved a rhexis size within 0.1 mm of target more often, as well as a greater rate of 360-degree capsulotomy coverage and 100 percent free-floating capsulotomies.6
Aperture CTC
“Manual capsulorhexis has been the gold standard for a long time now, but it’s still the most difficult step of the cataract procedure. Even in the best hands, there can still be heart-stopping moments,” says Mark Packer, MD, of Mark Packer MD Consulting in Boulder, Colorado, and chief medical officer of International Biomedical Devices in Mt. Pleasant, South Carolina. “One of my colleagues from London, Brian Little, and I published a paper7 several years ago about how to save some of these situations where the capsulorhexis goes astray. That actually became one of my most popular publications, somewhat to my surprise. But it shows that people are really in search of a better way to do this that has a higher success rate. Published studies show complication rates from 2 to 5 percent for manual capsulorhexis. So the idea is to achieve a more consistent, more reproducible and safer way of opening the anterior capsule.”
 |
| The Aperture CTC is a small red-orange laser that fires continuously instead of in pulses, controlled by a foot pedal when the flexible, disposable stainless-steel cutting element is in proper contact with the capsule. |
Dr. Packer’s company is attempting to answer that need with the Aperture CTC (“continuous thermal capsulotomy”), which consists of a console that provides constant energy to a single-use, stainless steel ring-shaped cutting element that retracts and re-opens to fit through a small incision and then contact the capsule 360 degrees around without suction. The disposable ring, integrated within a disposable handpiece that the manufacturer says feels similar to a phaco handpiece, comes in sizes ranging from 4.5 to 6 mm, in 0.5-mm increments. Thermal energy quickly cuts a free-floating capsulotomy; the surgeon easily retracts the loop with the cap and removes it through the entry wound for disposal.
“Essentially, it is a stainless steel circle that is stretched to a narrow ellipse that allows entry through what is currently a 2.4-mm incision, but further refinements may decrease that a little bit,” Dr. Packer explains. “Once inside the eye, it re-forms into a full circle. Then, by depressing the foot pedal, a very short pulse of electricity is sent through the device in milliseconds. Again, time span is one of the things we’re still toying with a little bit. As the thermoelectric current passes through the circle, the heating essentially surpasses the melting temperature of collagen, creating an instantaneous complete capsulotomy. Once that’s done, the circle is converted again into a very narrow ellipse that can be withdrawn from the eye, taking with it the central cap. The eye is then ready for surgery for the extraction of the lens.”
Dr. Packer thinks that the Aperture CTC is easy for surgeons to learn and safe for their patients. “I think it’s extremely easy,” he says. “It’s very intuitive. The user interface is very simple. There are a bunch of safety checks that are built into the circuitry so that you can’t really mess up. If anything is not connected properly, the device will let you know, and it won’t fire.” He adds that the disposable handpiece is suitable for right- or left-handed surgeons and just a little bit lighter than a phaco handpiece.
“We have an alignment mark in the center of the circle, which can be aligned with the Purkinje light reflexes, so if the surgeon wants to center on the optical axis, a line from the first Purkinje to the fourth Purkinje—or even the third Purkinje—that can be done,” he says. Unlike the Zepto, Aperture CTC doesn’t incorporate suction into making contact between the ring and the capsule. “We don’t need any vacuum: Basically, you just place the stainless-steel ring on the capsule,” he says. “It just has to be in 360-degree contact, and minimal downward pressure is needed.”
Although the manufacturer emphasizes the Aperture CTC’s potential niche as a less costly, easy-to-use femto alternative, Dr. Packer doesn’t see the emerging device—which will be in human trials later this year—as a competitor with femto. “As everyone knows, femtosecond lasers are very expensive and their use is therefore limited to the premium channel of refractive cataract surgery,” he says. “The cost is often a click fee of several hundred dollars, and so the only way that works is if the patient is paying for the advantages that accrue with femto, such as better astigmatism correction with toric axis guidance built into the laser, for example. Plus, the laser also performs other steps besides the capsulotomy. But it’s fundamentally a premium-channel device, and Aperture CTC is not. Although I can’t currently tell you exactly what the price point will be, our goal is to make it very affordable for routine cataract surgery so as not to add much cost to the procedure, and to perhaps even save some money by reducing the complication rate. So we’re not really competing with femto. I think femto will always have a role for refractive cases; we’re looking at this as a device for precision capsulotomy in routine, everyday cataract surgery.”
Dr. Packer says that he believes that one possible advantage the Aperture CTC may enjoy over manual capsulotomy is that the denatured collagen edges roll over on themselves for added smoothness and strength, a feature thought to be shared by the Zepto. “With the Zepto device, they noted that their capsulotomy was actually stronger than a manual rhexis, presumably because of the fact that when the capsulotomy is constructed, the edge of the capsule actually rolls over itself. We have seen that same constellation of findings,” he says. “The cut edge is actually facing away from the opening because it’s rolled back on itself. I believe that occurs because you’re heating the cut edge to the point where it cuts; but beyond that, it’s also that a little bit of heat is causing a tightening of the lens capsule.” Dr. Packer likens the tightening effect on the rhexis edge to what occurs in laser facial resurfacing. “You can see the collagen in the facial tissue tighten up when heat is applied. It constricts, and that’s what also strengthens the capsulotomy,” he says. REVIEW
Dr. Packer is the chief medical officer of International Biomedical Devices. Dr. Thompson is a researcher and consultant for Mynosys, and served as an FDA investigator for the Zepto trials. Dr. Taravella is consultant for Johnson and Johnson Vision-AMO for the Visx, and is a proctor for both the Visx and IntraLase lasers.
1. Mohammadpour M, Erfanian R, Karimi N. Capsulorhexis: Pearls and pitfalls. Saudi J of Ophthalmol. 2012;26:1:33-40.
2. Chang DH, Waring GO. The subject-fixated coaxially sighted corneal light reflex: A clinical marker for centration of refractive treatments and devices. American J Ophthalmol 2014;158:5:863-74.
3. Thompson VM, Berdahl JP, Salono JM, Chang DF. Comparison of manual, femtosecond laser, and precision pulse capsulotomy edge tear strength in paired human cadaver eyes. Ophthalmol 2016:123:265-74.
4. Kahook MY, Cionni RJ, Taravella MJ, Ang RE, Waite AN, Solomon JD, Uy HS. Continuous curvilinear capsulorhexis performed with the VERUS ophthalmic caliper. J Refract Surg 2016; 32:10:654-8.
5. Lee JH, Yong EL, Joo C. Clinical results of the open ring PMMA guider assisted capsulorrhexis in cataract surgery. BMC Ophthalmol 2018;18:1:116.
6. CAPSULaser. Latest CAPSULaser data presented at AECOS. https://www.CAPSULaser.com/latest-ce-data-for-CAPSULaser-at-aecos. Accessed 13 June 2018.
7. Little BC, Smith JH, Packer M. Little capsulorhexis tear-out rescue. J Cat Refract Surg 2006;32:9:1420-22.