It is important to be extremely accurate because, for every degree that the lens is off, the patient loses 3.3 percent of astigmatism correction. In other words, if the toric lens is off by 30 degrees, it has no effect. “One minute on a clock is 6 degrees. If you are off that much, 20 percent of the astigmatic correction of the lens is lost,” Dr. Devgan notes.
Measure
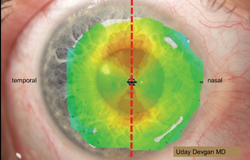
There are several ways to measure the axis of astigmatism. “Most ophthalmologists use a corneal topographer to measure the corneal axis, but what if the patient’s head is not straight during the measurement? If the patient’s head has a slight tilt to it, everything is going to be off because the measurement will be off. When measuring, the patient’s head must be absolutely perpendicular to the floor,” Dr. Devgan says.
To measure the axis of astigmatism, Daniel H. Chang, MD, in private practice in Bakersfield, Calif., first performs IOLMaster biometry on all of his IOL patients followed by Atlas corneal topography. “I do at least two different IOLMaster measurements on separate days,” he says. “That way, I can see if there is significant variability in the keratometry readings.
|

Mark
There are several methods for marking the axis of astigmatism, and they vary in accuracy. Since the approval of the first toric IOL, the standard of care for marking the axis has been ink. However, because of the precision required for both measuring and marking the target axis, ink pens are not ideal. “This is the least accurate method because it is a guesstimation,” says Robert H. Osher, MD, in practice at the Cincinnati Eye Institute. “The ink diffuses and may even completely disappear. Surgeons who rely on ink cannot have a very high degree of confidence that they have nailed the target meridian with the lens.”
He notes that surgeons are always aiming for precise toric lens alignment. “We have all of this sophisticated technology for removing the cataract and wonderfully sophisticated intraocular lenses to replace the cataractous crystalline lens. So, how can the international standard of care for aligning the toric lens be a $1 ink pen?” Dr. Osher asks.
Dr. Chang agrees that marking pens are not ideal. “They are okay, but the ink mark itself is wide,” he says. “These ink marking pens don’t have a microscopically fine tip. It’s more like a Sharpie. It makes a thick mark instead of a tiny pinpoint mark. Additionally, the marks bleed and can smear out after a while.”
|
Another method is using imaging or fingerprinting. “A picture is taken of the iris when the pupil is dilated during the original examination, and then software superimposes a protractor so every landmark on the iris or the limbus has the exact degree associated with it,” says Dr. Osher. “The surgeon can easily identify crypts, pigment, the vessels and the unique stromal patterns of the iris. A detailed photograph of the iris when the pupil is dilated, just like it is going to be in surgery, allows the surgeon to be confident about finding the target meridian. This is an accurate method that I introduced during the Kelman Innovator’s Lecture in 2009.”
To avoid the smearing or disappearance of an ink dot, Dr. Osher has developed Thermodot with BVI. “A probe leaves a tiny cautery dot that is placed at the limbus, signifying either the major meridia or where the target meridian is located,” he says. “The intraoperative version is available today, and BVI is planning to introduce a portable unit for marking in the preoperative area at ASCRS next year.”
The next method is limbal registration. “Basically, you take a picture of the limbus, and the technology memorizes it,” says Dr. Osher. “In surgery, you can use a thumb drive to re-create the image on a monitor or through the microscope and then overlay the digital degree marker. You can see the target meridian based on the captured registered image, and then it’s very easy to know exactly where to orient the toric lens. SMI (Germany) pioneered this technology, and Zeiss has developed its own registration software. Alcon bought SMI and is pioneering this approach in the United States with the Verion Guidance System.”
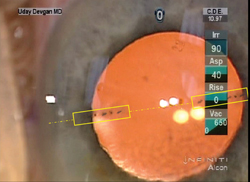
The last method is wavefront intraoperative aberrometry, and there are currently two of these systems: WaveTec’s ORA System with VerifEye and Clarity’s Holos. “An intraoperative refraction using wavefront aberrometry will identify where the cornea is steepest,” Dr. Osher says. “It takes into account both the anterior and posterior cornea and does not depend upon preoperative diagnostics. This technology provides a surgeon with information that allows rotation of the toric lens until it is precisely aligned. In addition, this sophisticated technology not only confirms the toric axis, but also confirms emmetropia. Intraoperative wavefront has the potential to confirm that both the sphere and the cylinder are corrected. Confirming emmetropia on the table is every ophthalmologist’s holy grail.”
Dr. Devgan notes that the ORA and Holos devices work well, but he says they will be even better after a few generations. “With aberrometry, after the toric IOL is placed in the eye, the machine indicates whether the lens needs to be rotated and how much,” he says. “If the lens needs to be rotated, that is done, and then placement is checked again. These systems work better in patients with larger amounts of astigmatism. The more astigmatism, the easier it is to measure. For mild degrees of astigmatism, these machines are less accurate. For more than 3 D of astigmatism, they are super accurate.”
Dr. Chang notes that it is not unusual for one side of the implant to match the axis mark while the other side does not. “If one set of marks on the implant matches the axis mark on the cornea and the other one does not, it is not immediately obvious which one is misaligned. The answer lies in the centration of the toric lens. I would prefer my toric lens to be centered, with the lens marks parallel to my limbal marks rather than to have my toric lens decentered and both sets of marks aligned. Therefore, I am actually trying to line up the two limbal corneal marks, the two marks on the implant and the center of the implant. Rotational accuracy is important because if there is malrotation, not only are you losing astigmatic effect, but you are also inducing astigmatism in another meridian,” he says.
Lens Placement
The last step is to keep the toric IOL in place after it has been implanted. According to Dr. Devgan, there are several pearls for achieving lens stability. First is to make the capsulorhexis so that it overlaps the edge of the optic. “If the optic is 6 mm wide, even if the capsulorhexis is 5 mm, it will shrink wrap down and really hold that lens very well. The second pearl is to remove all of the viscoelastic. After you put the lens in the eye, you’ve got to go behind the IOL with your I/A probe and suck out all of the viscoelastic because you want that lens to directly touch the capsular bag. If you leave viscoelastic in there, it acts as a lubricant and allows the lens to slip,” he explains.
It is also imperative to ensure that the incision is completely watertight. “If there is even a microscopic leak there, it may leak slowly over the next few hours. When the eye deflates because of a leak, the lens can rotate a little,” Dr. Devgan says.
|
Bausch + Lomb’s Trulign toric IOL has the advantage of four haptics. “That lens ends up being exquisitely stable in the eye. The haptics are made of polyamide, which is a material that glues itself to the capsular bag. That lens will not shift,” Dr. Devgan says.
According to Dr. Devgan, there are currently four FDA-approved toric IOLs: Staar toric, AcrySof, Trulign, and Tecnis. “Staar was the first one to enter the marketplace,” he says. “It is a single-piece plate haptic design made of silicone. It has two steps of correction. Next was the AcrySof lens, which is available in the most sizes and has seven steps of correction. B&L’s Trulign and AMO’s Tecnis toric are the newest lenses, and they each have three steps of correction available. More toric lenses will be coming out in the future, and these lenses are among my very favorites, because they absolutely deliver on their promise. There is very high patient satisfaction. The only caveat with toric lenses is that the lenses must be stable in the eye and the corneal astigmatism should be regular and symmetric.” REVIEW





