|
Last month, the Food and Drug Administration approved Bausch + Lomb/Technolas Perfect Vision’s Victus femtosecond laser for sale in the United States. Though there are femtosecond lasers here that are approved to create LASIK flaps, and others approved for anterior capsulotomies in cataract surgery, the Victus is the first that can do both. Theoretically, this dual-functionality gives surgeons more options in their practice, potentially yielding more bang for the buck. Here’s a look at the system’s features and the impressions of international surgeons who’ve used it.
How to Use It
As surgeons get acquainted with a new femtosecond laser, whether for use in LASIK or cataract, one of the steps they focus on the most is docking, since every laser does it a little differently and it’s so crucial to the success of the procedure. Victus users say the laser docks a little differently than other lasers surgeons may have used in the past.
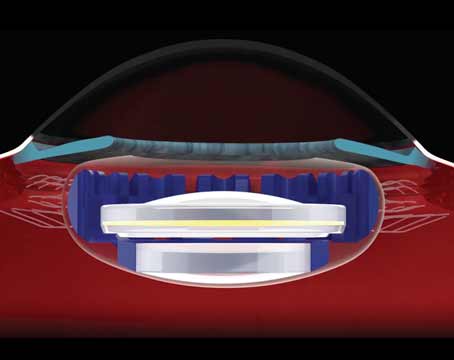
With the Victus, there are two pieces used for docking: a suction ring that is applied to the patient’s eye and a cone on the laser that fits into the ring. “The suction ring is very much like the Intralase’s, and we center it using a microscope,” explains Sheraz Daya, MD, medical director of the
Centre for Sight in London, England, and consultant to Bausch + Lomb. “We then add a few drops of either BSS or, in our case, tetracaine to the interface when suction is on and move the laser cone to the interface, docking it gingerly. We watch the process on OCT and an HD screen to monitor how far we’re going, because it’s a curved interface against a flat planar meniscus of fluid on the eye, so it’s quite common to get a bubble there. As soon as that bubble disappears due to bringing the cone closer to the cornea, we clip the ring onto the laser and that’s it. At that point, we make sure we’ve identified some fluid at least on the sides if not all the way across, meaning it’s kind of a semi-fluid interface.”
Chee Soon-Phaik, FRCOphth, an associate professor at the National University of Singapore and a B + L consultant, says the ability to use the system’s microscope during docking is unique, and can be a boon to some surgeons. “For surgeons who are more presbyopic, docking a femtosecond can be challenging since you have to do it without the aid of any magnification,” she says. “In the past, with other systems, I’ve seen surgeons who have had to use their cataract operating microscope to help them do the docking of their femtosecond. Here, we can use the Victus’ microscope to help get perfect docking by adjusting the magnification.”
One aspect of the system that could potentially change down the road is the Victus’ use of two joysticks for docking. “One is for controlling the x/y plane and one is for the z dimension,” explains Dr. Daya. “I actually asked for an omnidirectional one because I didn’t like to have to move my hand from one to the other constantly. I think they’re now working toward offering something like that in a variation of the current Victus.”
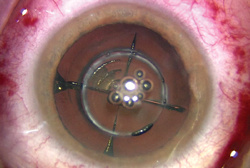
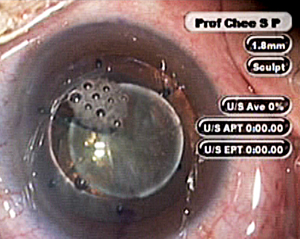
After the Victus is docked and the surgeon moves on to creating the capsulotomy, surgeons say the laser’s speed results in fewer bubbles being generated, which helps avoid undesirable outcomes such as tags on the capsulotomy rim. “One of the advantages is there are hardly any bubbles created that can block the beam,” says Dr. Daya. “It’s fast—80 KHz—and because it moves quickly the spot separation can be narrower and the energy reduced. When you reduce the energy, the bubbles created are smaller, leading to less accumulation of them and interference. It usually takes about 15 seconds to do the capsulotomy and lens fragmentation.”
Dr. Chee says the unit’s real-time optical coherence tomography can be helpful for monitoring the procedure in case an unexpected event occurs during the photodisruption. “You can see the bubbles appearing and fluid erupting as you treat with it,” she says. “This has proven helpful because we once aborted a case when something wasn’t proceeding correctly with the treatment.”
Dr. Chee says she’s demonstrated the strength of the femtosecond capsulotomy in a case of a subluxated lens. “I deliberately created an initial small capsulotomy in a subluxated lens that was displaced so far laterally you could see the edge of the cataract,” she says. “I then applied iris hooks on the capsule through the capsulotomy in order to pull the whole nucleus to the center so I wouldn’t see any vitreous. You probably wouldn’t be able to do that with a manually created capsulotomy.”
|
Devilish Details
Surgeons say though it’s true the laser can create flaps as well as perform other procedures that require an initial corneal lamellar resection, and can also perform anterior capsulotomies in conjunction with cataract surgery, putting both LASIK and cataract functions to use in a practice is not always easy. The problem stems from the fact that most surgeons in the United States perform LASIK in a non-OR procedure room at their office, but do their cataract surgeries elsewhere in a sterile hospital or ambulatory surgical center environment. The Victus can only be in one location, however.
“For us, the rooms are next to each other, but even then it’s a logistical problem,” says Dr. Daya. “I suppose that if we start having a lot of cataract work, we’ll dedicate one machine to doing the cataract steps. One Czech surgeon, Pavel Stodulka, uses three rooms: one in which someone does all the femto work on the Victus and two others outfitted for cataract surgery. Dr. Stodulka then alternates between the two surgical rooms as he’s being fed patients from the Victus room. If you only have two rooms, what might be efficient would be to have a laser suite with the excimer and femtosecond and then have an adjacent cataract room. You could possibly do three Victus patients at a sitting and then do their cataract procedures afterward.
“It’s possible to do it all in one room,” Dr. Daya says. “At one of our low-volume centers, there are lasers and a cataract OR in one room. For a single-surgeon practice or a small group, you could do a day of refractive and cataract surgery and spend the day in that room. It all depends on what sort of volumes you have, your practice model and your available space in your center. In the end, it’s all part of the learning curve, isn’t it?”
REVIEW