Since the development of anti-vascular endothelial growth factor injections, they’ve become the standard treatment for age-related macular degeneration, macular edema, diabetic retinopathy and retinal vein occlusion. Though physicians are adept at performing the injections, there’s always the risk for a possible complication. The use of intravitreal injection guides can potentially reduce subconjunctival hemorrhage while ensuring patient comfort.
“There are basically three functions that the guide should fulfill: First, to expose the injection site,” says, Harvey Uy, MD, medical director of Peregrine Eye and Laser Institute at the University of Philippines. “The second function is to identify the site of the injection, which is typically around 3.5 mm from the limbus. Thirdly is to allow you to inject at a set depth so that it limits the depth of the needle incursion.”
Here, we’ll take a look at some of the available injection guides.
Precivia (FCI Ophthalmics)
 |
|
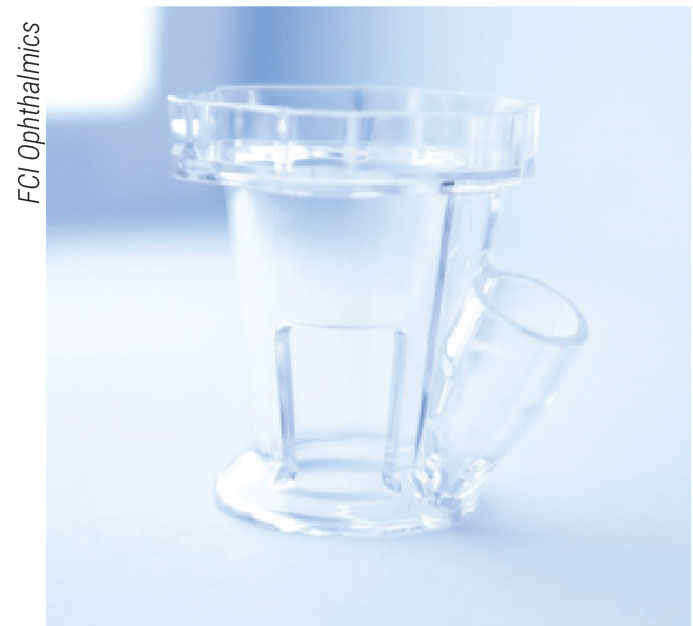
A faint line down the side of the Precivia device to the base of the guide tube can help physicians better position the device properly on the limbus. |
Precivia, originally called InVitria, is a single-use intravitreal injection guide from FCI Ophthalmics. This is a clear-plastic device placed on the patient’s eye without the need for a speculum, caliper or pressure plate. A guide tube with a fixed angle of 28 degrees and a fixed distance of 3.5 mm from the limbus allows ophthalmologists to safely inject without losing the position of the injection site. The cylindrical design has a rigid handgrip at the top for easier placement and stabilization, and the rounded base ensures that both eyelids are positioned properly for injection, the company says.
According to FCI, by gently pushing down and rotating the Precivia device, the eye becomes stabilized, which will create an anesthetic effect for the patient due to the pressure. Also, after the device has been positioned, the patient won’t be able to see when the needle is coming. After the needle is removed, by rotating the device again post-injection, the conjunctiva is replaced, and the injection hole is sealed.
In a prospective review of 200 intravitreal injections, 100 using Precivia and the other 100 using traditional methods, surgeons’ perceptions and patients’ intraoperative visual analogue scale (VAS) pain scores were recorded. The average VAS pain score in the Precivia group was 1.38 compared to 2.58 in the traditional group, which was statistically significant. Additionally, surgeons reported that insertion using Precivia was easy in 89 cases, moderate in 10 cases, and difficult in one case. The surgeons added that the device offered excellent globe stability and a safe, reproducible entry site and angle needle insertion.1
Rapid Access Vitreal Injection (RAVI) Guide (Katalyst Surgical)
 |
|
Developers of the RAVI Guide noted that as the needle is withdrawn, the base plate may be slid over the conjunctiva to close the injection site if needed. |
The Rapid Access Vitreal Injection Guide is a reusable, metal intravitreal injection guide. A baseplate at the end of the handle measures 7 mm by 7 mm. Two flanges on opposite sides of the baseplate hold the ocular structure, creating an injection site with a distance of approximately 3 to 4 mm from the limbus. After setting the device onto the ocular surface, the physician can safely make an injection through the 1.5-mm diameter aperture in the center of the baseplate.
The inventors of the RAVI Guide noted that the device can replace the function of both a lid speculum and caliper. In a prospective study to evaluate their device, the inventors along with a team of physicians performed 54 intravitreal injections using either the RAVI Guide or a lid speculum. They wanted to study patient acceptance of the device, complication rates and operative goals.
During the study, researchers had patients use the Wong-Baker FACES pain scale to rate their intraoperative treatments. The scale allows patients to choose from zero (no pain or discomfort) to 10 (severe levels of pain and discomfort), along with illustrated faces depicting emotions ranging from happy to sad. This simple rating scale helped researchers understand patient acceptance of the RAVI Guide compared to the speculum. In the RAVI Guide group, 72 percent (n=32) of patients had a pain-free experience compared to 64 percent (n=22) of patients in the speculum group. A pain score of two or higher was reported in 16 percent of RAVI Guide patients and 32 percent of speculum patients.2
Researchers reported that operative goals to safely inject anti-VEGFs were achieved in all patients, and there weren’t any significant operative complications observed for either device.2
Doi-Uematsu Intravitreal Injection Guide (Duckworth & Kent)
 |
The Doi-Uematsu Intravitreal Injection Guide is a reusable guide suitable for right-handed surgeons, as the guide’s handle was designed to be held in the left hand leaving the right hand free for needle insertion. At the base of the handle is a 12-mm diameter ring with a “snow-tire” pattern for a firmer grip on the ocular surface and increased stabilization. According to D&K, there’s a 5.5-mm break in the ring that enables an anterior chamber tap, if required, in order to avoid intraocular pressure spikes. The guide hole is 0.5 mm in diameter, which is suitable for 27-gauge or smaller needles. This device is autoclavable.
Researchers who designed the device conducted a retrospective review to compare the safety and efficacy of the guide. The study included 256 patients who underwent 992 intravitreal anti-VEGF injections over a two-year period. Of the total injections, 907 were done using the intravitreal guide, while 60 were done without it. A remaining 25 injections weren’t determined ahead of the study. Overall, local complications in the guide group consisted of one case of uveitis, one case of retinal tear and one case of amaurosis fugax. There were no local complications in the non-guide group. Researchers reported no major complications during the study. The researchers say that though all complications occurred in the Doi-Uematsu Guide group, the difference between groups wasn’t statistically significant.3
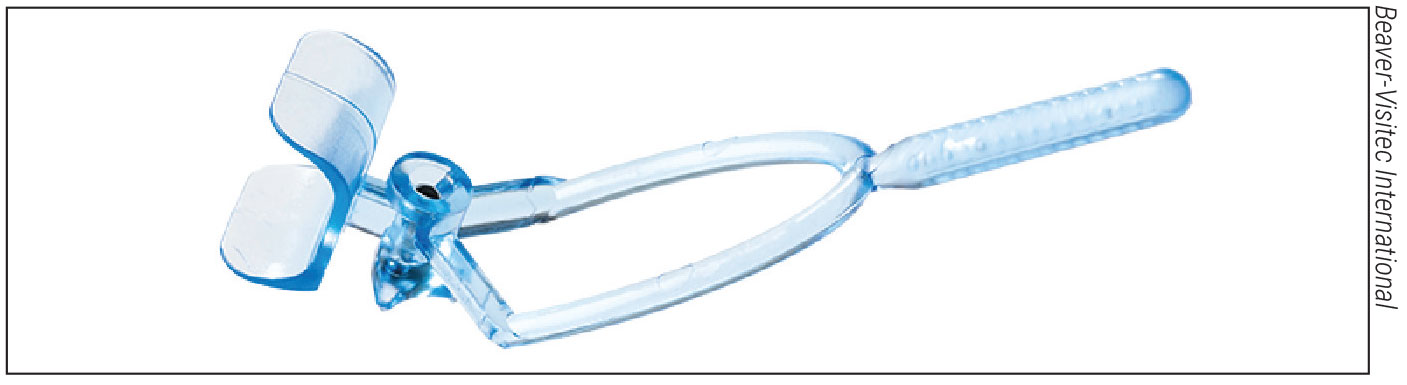
Malosa Intravitreal Injection Guide (Beaver-Visitec International)
The Malosa Intravitreal Injection Guide, designed by UAE surgeon Salman Waqar, is a single-use injection guide. According to Beaver-Visitec International, the guide is designed with a polycarbonate lash guard and a stainless-steel guide tube. The handle is shaped like a wishbone and positioned at a 45-degree angle to increase stabilization and ensure that it doesn’t become a disturbance during treatment.
“Aside from helping you inject anti-VEGF drugs, you can use it to guide you for injecting other medications such as antibiotics, for example, and it can also be used to help someone extract vitreous material from the posterior segment,” says Dr. Uy.
“Sometimes in an effort to further decrease patient discomfort, we might use a smaller needle,” continues Dr. Uy. “Typically, we use a 30-ga needle, but sometimes we can transfer the drug through a 31-ga needle. That’s smaller so it’s more comfortable, and sometimes before injecting triamcinolone—which is not a liquid but more of a suspension—we will use a larger-bore needle, like a 27-ga needle, so that we can inject the suspension more easily. And both the smaller and larger needles will go through the Malosa guide without difficulty.”
 |
|
Dr. Salman Waqar, is the inventor of the Malosa Intravitreal Injection Guide. He sought to design a device for rapid, safe and precise delivery of injections without using a technique needing drapes, calipers and speculums. |
Dr. Uy and his colleagues conducted a clinical trial observing 200 adult eyes undergoing intravitreal injection treatment. “We found two additional benefits when using the Malosa: One is that the patients report less pain compared to using the standard dual-blade eyelid retraction device,” says Dr. Uy. “Secondly, we saw less subconjunctival hemorrhage.”
During the study, 100 eyes were assigned injections using the Malosa Guide, and the other 100 eyes received treatment with a conventional dual-blade speculum and a surgical caliper. The study sought to compare the mean procedural time and complications when using either the guide or a speculum and caliper. The mean procedural time was shorter in the guide group (9.94 ±2.87 seconds) versus the speculum group (21.85 ±7.25 seconds). Dr. Uy reported that the rate of post-injection subconjunctival hemorrhage was higher in the speculum group, for which he had no explanation. No other injection-related adverse reactions were observed in either of the patient groups.4
“Physicians’ workloads are very heavy, especially with regard to the need to inject a lot of patients,” says Dr. Uy. “However, injections shouldn’t hinder physicians’ work of seeing patients and doing other procedures in the clinic. So, if we can find a way to minimize the time to do the injections, that’ll make our workflow more efficient.”
Dr. Uy has no financial interests to disclose.
1. Ratnarajan G, Nath R, Appaswamy S, Watson S. Intravitreal injections using a novel conjunctival mould: A comparison with a conventional technique. British Journal of Ophthalmology 2013;97:395-397.
2. Han DP, McKenney KC, Kim JE, Weinberg DV, Singh RSJ. Clinical evaluation of the Rapid Access Vitreal Injection (RAVI) Guide: A hand-held instrument for assisting intravitreal injections. Invest. Ophthalmol Vis Sci 2016;57:12:2673.
3. Watanabe K, Masafumi U, Mohamed YH, Watanabe T, Doi Y, Azusa F, Kitaoka T. Safety of intravitreal injection guide. Journal of VitreoRetinal Diseases 2018;2:1:26-31.
4. Uy HS, Artiaga JCMComparison of two different intravitreal injection techniques. Clin Ophthalmol 2021;15:2383-2389.


