The system is a small addition to a microscope that allows the surgeon to overlay aiming reticules onto the image of the eye. By using these reticules as guides, Dr. Perez says, the surgeon can ensure the correct diameter of the capsulorhexis as he creates it.
"If you're operating on a high myope, for example, the eye is large, so 6 mm doesn't look very big," he says. "But if you're operating on a hyperopic eye, which is smaller, a 6-mm diameter would look different. You can't adjust based solely on your intuition."
The sizes of the circles automatically scale up or down if the surgeon zooms the microscope, and can also be turned on or off. The device can also put axis marks on the image, to help in centering a toric IOL.
Dr. Perez believes such capsulorhexis precision is required more and more with the advent of multifocal IOLs.
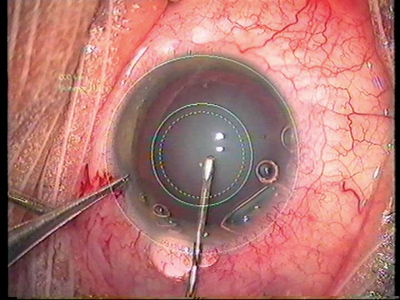 |
| Aiming reticules projected onto the microscope view aid the surgeon in making a capsulorhexis that's customized for the diameter of the IOL. |
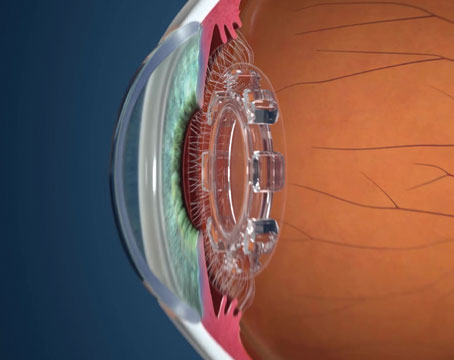
"The ReStor IOL, for example, has a 6-mm optic, with the inner rings used for near and vision and the peripheral mainly for distance," Dr. Perez says. "The problem is, if you make a small 4-mm capsulorhexis, the optical function of the periphery of the IOL will be limited, since the capsulorhexis will be hiding part of the lens."
When Dr. Perez operates, since most IOLs have 6-mm optics, he generates three aiming rings: one on the limbus; a smaller one that's the diameter of the IOL, which is
6 mm in most cases; and then an even smaller one at 5.5 mm. He then knows that if he keeps his capsulorhexis between the 5.5- and 6-mm rings, it will be custom fit for the 6-mm optic. He says this slight overlap helps decrease posterior capsular opacification postop.
As evidence of the benefits of overlapping capsulorhexes, he recounts a study he presented at the American Society of Cataract and Refractive Surgery. In the study, he divided 300 cataract-surgery patients into three equal groups. One group got the Alcon Acrysof, the second received a hydrophilic IOL from the French company IOLTech, and the third group received AMO's Sensar lens. They took a photo of each patient's capsulorhexis during the first postop week, noting whether their capsulorhexes were decentered (overlapping in some areas of the lens periphery, but not all), very large (beyond the optic size), or slightly overlapping the edge of the IOL ("customized"). He followed them for three years.
He says the eyes with customized capsulorhexes did best in terms of slowing down the progression of posterior capsule opacification, no matter what style of IOL they had. He says this is because the bags with the customized capsulorhexes heal evenly, avoiding wrinkles that draw cells toward the center. The custom tears may also seal the capsule in the periphery of the lens, helping prevent cell migration.