Treating Resistant Ulcers
CXL is showing benefit as a means to prevent complications and promote healing when corneal ulcers are otherwise non-responsive to standard antibiotic or fungal treatment. This use of CXL technology is called PACK-CXL (Photo-Activated Chromophore for infectious Keratitis cross-linking).
Farhad Hafezi, MD, PhD, chair and professor of ophthalmology at the University of Geneva, Switzerland, and clinical professor of ophthalmology at the Doheny Eye Institute at the University of Southern California, Los Angeles, has been using this approach since 2007. His group published the first paper on this procedure in 2008.1
Recently, Dr. Hafezi and colleagues conducted a randomized, prospective clinical trial involving 40 patients at clinics in Egypt, the UK and Switzerland with advanced infectious keratitis and corneal melting (Ophthalmology 2014, in press). Twenty-one eyes were treated with both antimicrobial therapy and PACK-CXL; 19 control eyes received only antimicrobial therapy. The size of the corneal ulcers was significantly larger in the PACK-CXL group: 5.62 ±1.88 x 6.22 ±1.98 mm, vs. 3.97 ±2.5 x 4.22 ±2.18 mm.
Mean duration to complete healing was 39.76 ±18.22 days for the PACK-CXL group and 46.05 ±27.44 days in the control group (not significant: p=0.68). Three patients in the control group (21 percent) developed perforation; one had an infection recurrence.
|
Possible Mechanisms
Dr. Hafezi explains there are three possible mechanisms that might account for the benefits seen when using PACK-CXL. “The first possibility is direct intercalation of the chromophore to the DNA of the pathogen, causing irreversible binding and suppression of replication,” he says. “A second possibility is that generation of reactive oxygen species during the process destroys the cell walls of the pathogens. A third possibility is that changes in the three-dimensional structure of the collagen fibers make it harder for collagenases, which are upregulated during corneal melting, to dock and exert their action.”
Dr. Hafezi notes that the use of CXL to address resistant corneal ulcers is not yet widespread. “This is still in the pilot phase,” he says. “I would compare it to the use of CXL to address keratoconus back in 2002. Proof of concept had been given, but it had not caught on yet.”
Dr. Hafezi says it’s not yet clear what conditions might contraindicate this use of CXL, or whether there is a downside to the treatment. “We observed a slight increase in the size of a hypopyon in one patient,” he says. “When thinking about it, this seems logical: We killed a lot of pathogens simultaneously, so the size of the hypopyon had to increase immediately postoperatively. A similar reaction has been seen in the treatment of tuberculosis, where it’s called a Jarish-Herxheimer reaction.”
Dr. Hafezi believes this use of CXL may become more important than treating keratoconus. “I believe that PACK-CXL will have a much greater impact on global ophthalmology,” he says. “It addresses the third leading cause of global blindness—corneal infections, according to the World Health Organization—rather than a rare disease like keratoconus or postoperative ectasia. However, to reach that point we have to make the treatment faster; we have to move the treatment out of the operating theatre; and we have to make this type of technology inexpensive so that everyone can have equal access to it. My research group is working to address all three of these concerns.”
Correcting Refractive Error
CXL is also being investigated as a nonsurgical method for correcting refractive error. Avedro, a company based in Waltham, Mass., recently received the CE Mark in Europe for its KXL II system, which can be used to deliver user-specified CXL patterns, including patterns designed to alter the patient’s refraction.
William J. Dupps Jr., MD, PhD, who performs cornea and refractive surgery at the Cole Eye Institute in Cleveland and is director of the Ocular Biomechanics and Imaging Lab at the Cleveland Clinic, has been researching CXL for many years. “We published a paper in 20112 that tested the concept of doing focal treatments with CXL, to see if we could leverage the shape change more specifically,” Dr. Dupps explains. “In computational models, we decentered the treatment toward the steepest part of the cornea and manipulated the treatment parameters to enhance the results. The modified treatments showed double or triple the topographic improvement achieved in the same models with a standard treatment.”
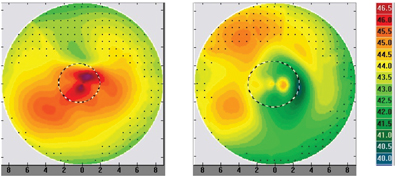
Dr. Dupps is now collaborating with John Kanellopoulos, MD, in Athens, Greece, who has been performing customized CXL on patients since it was approved in 2013. Dr. Kanellopoulos’s clinical work is bearing out what Dr. Dupps and his team observed in their modeling research. For example, one of his recent keratoconus patients was treated using a focal approach—without debriding the epithelium—and the result was a 5.5-D flattening of the cone, rather than the 1- or 2-D flattening that would be considered a very favorable result with a standard procedure. Other cases have produced similar results.
“Corneal tissue treated with CXL displays a focal flattening effect, not unlike that caused by a corneal scar,” Dr. Dupps continues. “By placing that zone of flattening carefully, changing the shape of the zone and adjusting other parameters like the depth of the treatment and the dosing of the light, we can customize the refractive result we achieve. The work done so far—both in the lab and with live patients—has shown that using CXL to correct refractive error is feasible.”
Does the effect last? Dr. Kanellopolous has observed that results are consistent over a six-month follow-up. Over the long-term, Dr. Dupps says data from earlier cross-linking trials may provide a tentative answer. “In the first published clinical trial, reported in 2003, patients were followed for as long as four years,” he says. “What shocked a lot of people was that instead of seeing loss of effect and progression of the disease after the first several months, the data showed an ongoing flattening effect in 70 percent of patients.3
“This wouldn’t necessarily be desirable in a refractive correction, of course, but these treatments treated the entire cornea and they treated diseased corneas, so it’s not clear that this would occur to the same extent in an otherwise healthy cornea,” he says. “One concept that’s been discussed as a means to address this is using a stabilizing treatment to lock in the refractive change you create. Such a treatment is under development.”
Dr. Dupps says the process of titrating the exact amount of correction created by a treatment requires ongoing study. “A bigger question is, what’s the maximum effect we’ll be able to achieve?” he notes. “We have a paper in press that describes computer simulations of what happens if we use different patterns and intensities to treat astigmatism, starting with tomographic maps of real patient eyes. A modest amount of corneal stiffening produced astigmatic corrections between 1 and 3 D. Most eyes with astigmatism fall within that range, and it’s possible to generate greater levels of corneal stiffening than we simulated.”
Dr. Dupps believes that within a few years this approach to refractive correction could give LASIK a run for its money—particularly in some patient groups. “I think many patients with lower refractive error would find it attractive to have an option that doesn’t involve removing tissue from the cornea,” he says. “And for patients who might be suspects for keratoconus, a treatment that stiffens the cornea while correcting refractive error would make a lot more sense than one that could potentially tip the balance toward ectasia by destabilizing the cornea.
“As a standalone treatment, the range of refractive correction will be more limited than some other procedures,” he adds. “But there are a lot of people living with low to moderate refractive error, and refractive CXL offers a completely different treatment paradigm for correction.” REVIEW
Dr. Dupps is listed as an inventor on related modeling technology being developed at the Cleveland Clinic. He serves as a consultant for Ziemer and has received research support from Zeiss, Avedro, NIH and The Ohio Third Frontier Commission. Dr. Hafezi has no financial connections to any products mentioned.
1. Iseli HP, Thiel MA, et al. Ultraviolet A/Riboflavin Corneal Cross-linking for Infectious Keratitis Associated With Corneal Melts. Cornea 2008;27:590-94.
2. Roy AS, Dupps WJ Jr. Patient-specific computational modeling of keratoconus progression and differential responses to collagen cross-linking. Invest Ophthalmol Vis Sci 2011;52:12:9174-87.
3. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol 2003;135:5:620-7.


