Small pupils have traditionally posed a challenge to surgeons. Miosis during cataract surgery limits visualization, makes it more difficult to access the cataract and increases the chances of iris damage.1 Patients may experience increased levels of postoperative iris inflammation and iris defects, which can sometimes lead to visual disturbances or photophobia.1,2 Increased vitreous loss has also been associated with poorly-dilated pupils, as well as posterior capsular rupture, irregular pupil shape and retained lens material.2 Luckily, pupillary expansion devices have all but eliminated complications, experts say. Here, we’ll peer into small-pupil cataract surgery and review some of the newer devices on the market that help make the procedure more manageable.
A Thing of the Past
 |
Before the advent of pupillary expansion devices, sphincterotomies and pupil stretching were used to manage small pupils. “We used to stretch the iris with two instruments or make incisions into the iris sphincter,” says Alan Malouf, MD, a surgeon at the University of Maryland Capital Region Surgery Center in Bowie and associate clinical professor at the UM School of Medicine. “The iris contour remained round, but some mobility was lost.”
“It was very easy in the days before pupillary expanders to get the iris caught in the phaco device,” says D. Michael Colvard, MD, FACS, of the Colvard-Kandavel Eye Center in Los Angeles and clinical professor of ophthalmology at the Keck School of Medicine of USC. “I recall occasionally seeing patients with tonic and distorted pupil margins who clearly had intraoperative trauma associated with small-pupil cataract surgery,” says Dr. Colvard. “Fortunately, this complication is rare now.” He says he’s seen a significant decrease in postoperative iris distortion since pupillary expansion devices have come to market. “Pupillary expanders have taken one of the most difficult and worrisome challenges in anterior segment surgery—the small and constricting pupil—and turned it into a non-issue,” Dr. Colvard says. (Incidentally, in terms of Medicare reimbursement, mechanical stretching of the pupil qualifies as complex cataract surgery, but there’s no additional payment for the pupillary expansion device itself. The device is included in the facility fee reimbursement.)
Causes of Small Pupils
 |
Alpha blockers, glaucoma, pseudoexfoliation and Flomax may lead to small pupils, says Dr. Malouf. He says there’s not much you can do preoperatively if pupils don’t respond to dilating drops, except to give a few extra drops. And in the case of Flomax, he says, “We don’t recommend that patients stop their Flomax before surgery. There’s no point in subjecting someone to urinary retention. ”
Chronic anterior segment inflammation with or without synechiae and intraoperative floppy iris syndrome, most frequently associated with prior use of alpha-1 adrenergic antagonists, are also common culprits causing poor pupillary dilation, adds Dr. Colvard. He says that if pupil dilation is suboptimal after topical and intracameral mydriatics, he turns to pupillary expansion devices.
Small-pupil Cataract Surgery
 |
Dr. Colvard begins every case with intracameral instillation of 0.2 to 0.5 ml of a solution containing 1.5% phenylephrine. If he has a patient who’s been on alpha-1 blockers but the pupil dilates widely with topical mydriatics, he says he feels comfortable proceeding after also injecting the intracameral mydriatic. “I’m convinced this helps enormously to stabilize the pupil and iris,” he says, “even in potential IFIS cases, as long as the pupil dilates well after topical mydriatics. If the pupil looks one bit ‘iffy,’ though, I put in pupillary expanders. The pupils that don’t dilate well are the ones that tend to come down and act floppy.
“In eyes with pseudoexfoliation that dilate poorly, I try to stretch the pupil, which is often hyalinized,” he continues. “In eyes with previous anterior segment inflammation, I lyse any posterior synechiae, but after this, if the pupil doesn’t dilate very well, I put in a pupillary expander.”
Hooks and Rings
“All pupillary expansion devices are pretty similar,” Dr. Malouf notes. Each ring is designed to expand the iris by pushing it outward, in contrast to iris hooks, which pull on the iris to dilate the pupil. The ring design allows for more even distribution of tension on the iris. “Hooks may be slightly more stressful,” Dr. Malouf says. “With hooks you have to titrate the tension, going around and pulling gently until it’s just right—you can’t just go in and pull them all the way out at once.”
 |
Another advantage of pupillary expansion rings is that you stay within your own incision, Dr. Malouf adds. “Each hook requires its own incision, but with the ring, you don’t need additional incisions.” Dr. Malouf says he almost always uses pupillary expansion rings if further dilation is needed. His choice of ring depends on what’s available at his surgery center.
Though pupillary expansion rings have certain advantages over hooks, Dr. Malouf doesn’t see them replacing iris hooks any time soon. For example, if a patient has asymmetric constriction or post-traumatic pupil, he won’t use a ring. “I think there will always be a role for hooks,” he says.
“The one instance when I prefer to use iris hooks is when I’m doing an IOL exchange,” says Dr. Colvard. “The iris hooks can be positioned to stay out of the way during an exchange, and you can ‘customize’ the pupil opening to allow better visualization in certain critical areas. The iris hooks take more time to position than intra-pupillary expanders, but with IOL exchanges, I find the time is well spent.”
Jeffrey Whitman, MD, chief surgeon at the Key-Whitman Eye Center in Dallas, points out that pupillary expansion rings take less time to insert and remove than iris hooks. Though the time difference isn’t too significant, experts agree that a faster method with fewer incisions can be very useful. “Most of the time, I’ll use four hooks,” Dr. Whitman says. “It takes a certain amount of time and skill to put each one in—and depending on where you put it, a hook might get in the way of your main phaco incision. Hooks are more useful to me if I need just one segment of the iris pulled out.”
Here are some of the latest offerings in the pupil-expander arena.
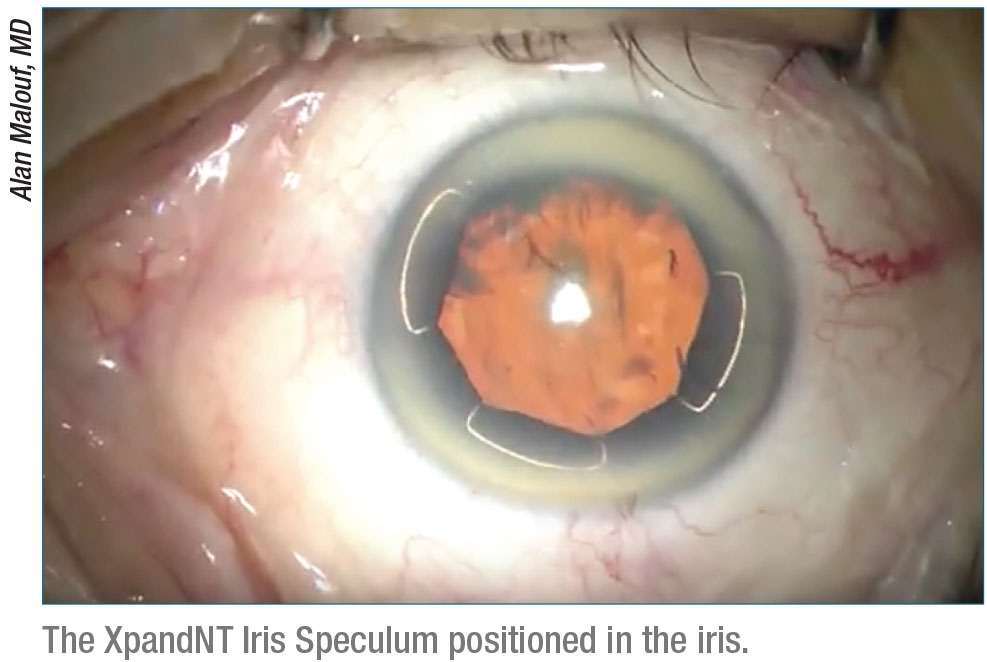
XpandNT Iris Speculum
The XpandNT Iris Speculum (Diamatrix) is a biocompatible, 0.003-inch-diameter laser-welded nitinol wire ring with 0.8-mm pockets that cradle the iris rim. XpandNT has eight points of contact, which the company says reduces iris trauma and results in a more circular pupil postoperatively. This ring creates a 6.7-mm aperture of near-circular dilation, and Diamatrix says it offers stability for IFIS, a clear pathway for instruments and is intuitive to place and rotate.
 |
Each package comes with four X1 injectors, each preloaded with an XpandNT Iris Speculum. The single-use injector features a tapered cannula for a 2.4-mm or greater incision and an easy-release manipulator tip. (Multi-use XpandNTs approved for up to five uses aren’t approved in the United States.) The injector tips are polished to provide little resistance, and because of this, the company advises surgeons to advance the injector plunger slowly. To remove the device, Diamatrix recommends Daniel Bregman, MD’s, two-step technique, which can be viewed at youtu.be/xnas6g9KmsQ.
Dr. Malouf appreciates the thin profile of the XpandNT and the wide dilation it offers. He says taking your time to carefully insert the ring pays off. “Because of its size and its metal frame, sometimes one of the flanges will get caught deep in the anterior chamber angle, and you have to fish it out,” he says. “But I don’t see that as a major disadvantage. It’s essential that you have the widest possible pupil for cases of very hard cataracts or if you need a big capsulotomy.” You can view a video of Dr. Malouf using the XpandNT at youtube.com/watch?v=AFnwThJjIN8.
Iris Expander
The Iris Expander (Oasis Medical), comes in 6.25-mm and 7-mm ring diameters and is made of a polypropylene material with four pockets that cradle the iris. The disposable, single-use, sterile Iris Expander is sold in units of five and is implanted using its own injector, which is also disposable. Oasis says the Iris Expander provides stable mydriasis during cataract surgery with no need for additional paracenteses. Capsulorhexis, hydrodissection, phacoemulsification and IOL injection can all be performed with the device in place, adds the company.
Dr. Whitman has used the Iris Expander in the past. He says he hopes Oasis will make the plastic material smoother and more flexible in the future.
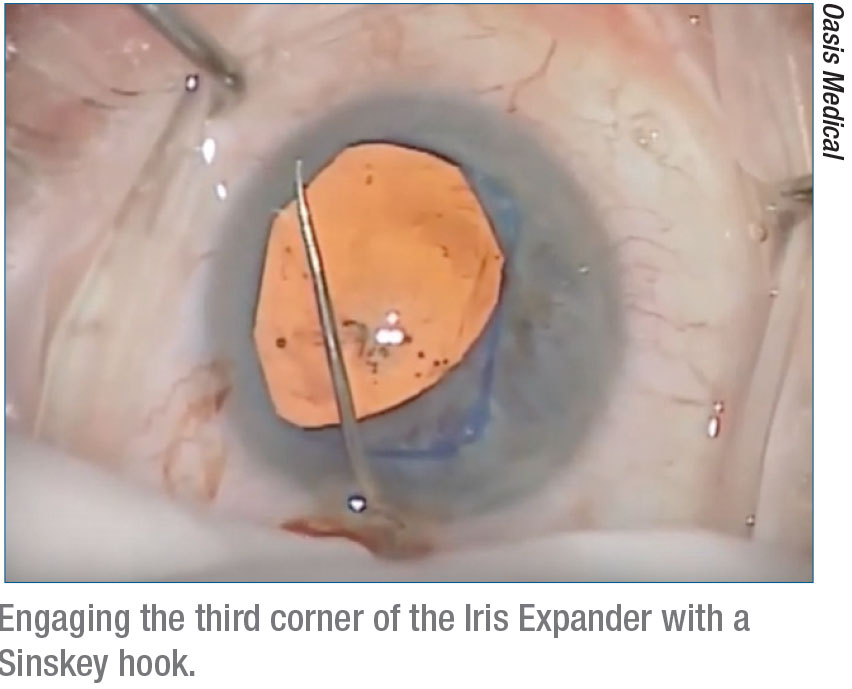 |
In a 2012 video demonstration, Dr. Whitman notes that the Iris Expander can fit through a 2.4- to 2.6-mm incision. He adjusts the ring with the help of a Sinskey hook and notes that “you’ll see iris edge at the corner after the insertion of each corner of the dilator. This is normal; this is what you should see.” To remove the Iris Expander, the surgeon pulls it directly out of the anterior chamber through the main incision. In the video, Dr. Whitman recommends using a collar-button type instrument to disengage the ring and pull it out.
The company also makes a stainless steel Iris Manipulator for the Iris Expander. It’s a double-ended instrument with a Sinskey hook at one end and a collar-button type instrument on the other.
You can watch the video of Dr. Whitman using the Iris Expander during cataract surgery here: youtube.com/watch?v=ea7fdK9TIxk.
I-Ring
Beaver-Visitec International’s I-Ring offers a 6.3-mm field of view for cataract, glaucoma and retinal surgery. It’s sold in packs of six, and each unit contains one ring and one injector. The green-colored ring, made of polyurethane, is described by the company as “soft, resilient and gentle on tissue.” BVI says its green hue makes for better visibility and contrast, and the fixed channel height helps to avoid compression and iris pinching during insertion and removal. It’s designed to remain planar in the anterior chamber to protect the corneal endothelium. BVI emphasizes that the I-Ring engages the iris at 360 degrees, eliminating even the smallest stress points.
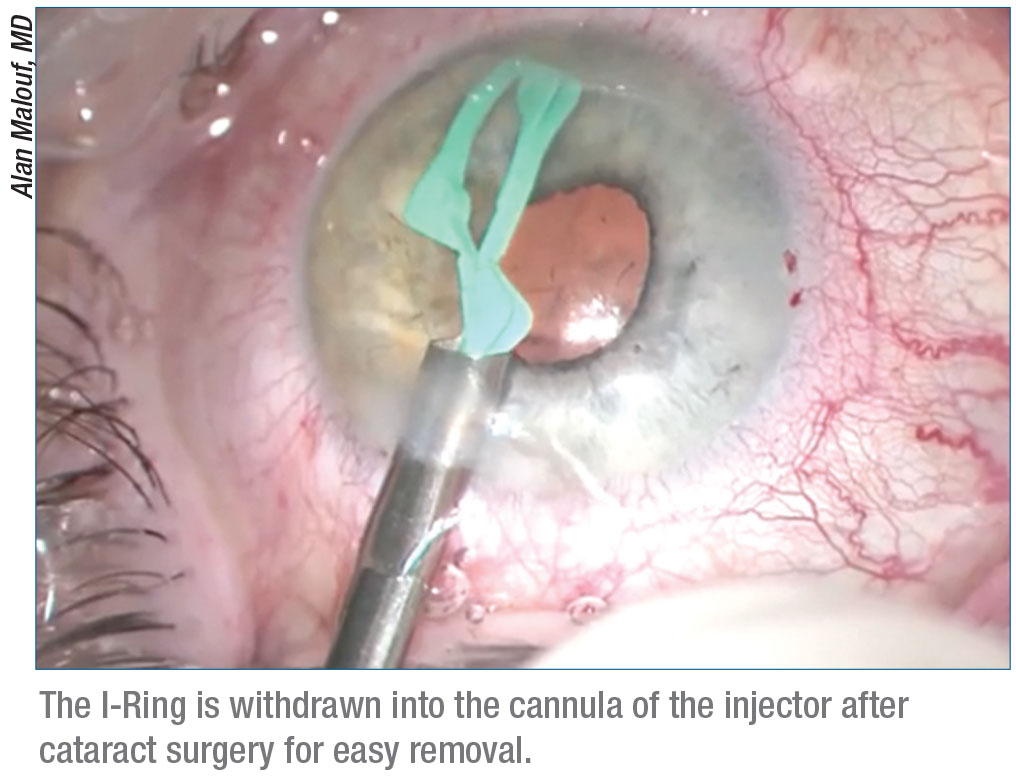 |
Dr. Whitman says he appreciates the easy insertion and removal of the I-Ring, which can be accomplished with the injector device. “The plastic in the I-Ring is very smooth, and the material is flexible,” he says. He notes that he’s never had an I-Ring crack or break in the eye.
Some surgeons have said the I-Ring has a high profile, compared to other rings, but Dr. Whitman says this would only matter if the ring got in the way of the procedure. “I shoot my lens implant through it, and I phaco with it in there,” he says. “It doesn’t impede any of my procedures. Another benefit is that I can use an I-Ring without disturbing the capsule even if I’ve done a femtosecond laser anterior capsulotomy. A lot of people think it’s too late to put the ring in once you’ve done femto because it’s engaging the capsulotomy edge and pupil at the same time.”
You can view a video of Dr. Malouf using an I-Ring for a brunescent cataract procedure here: youtube.com/watch?v=ABM2zf6oJ5Y.
Malyugin Ring 2.0
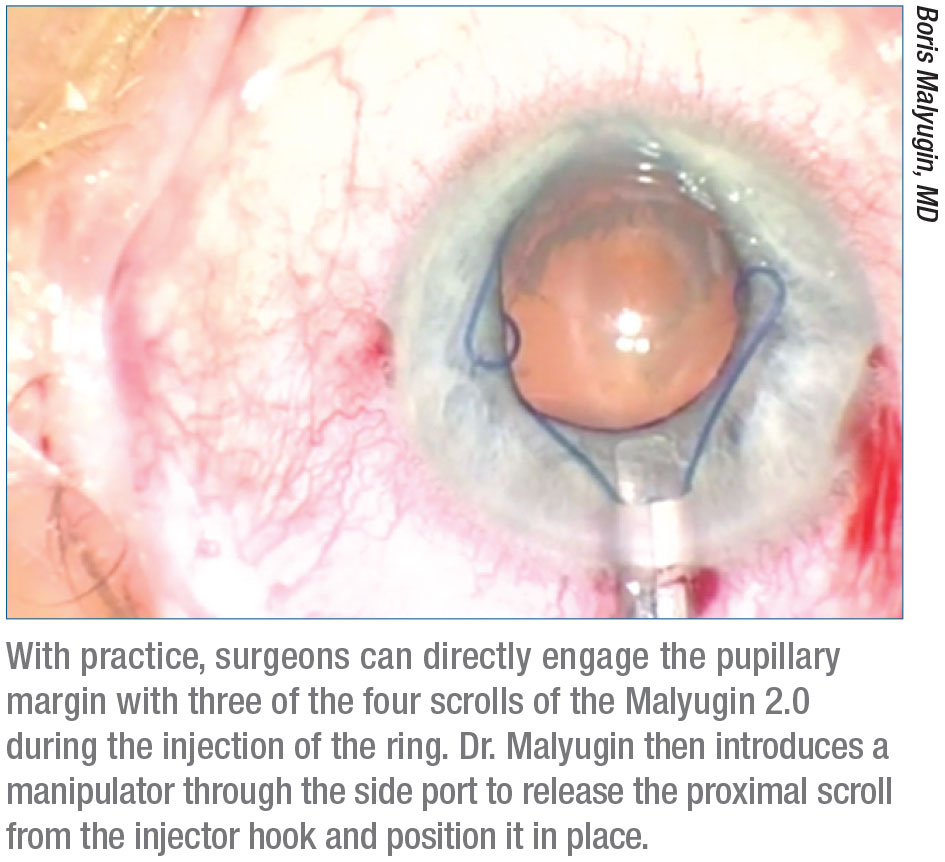 |
Designed by Boris Malyugin, MD, professor of ophthalmology at the S. Fyodorov Eye Microsurgery Complex in Moscow, the Malyugin Ring 2.0 (MicroSurgical Technology) is designed to be stronger and more flexible than the previous model. The ring is named 2.0 not only because it’s the second version, but also because this new model was redesigned to fit through a 2-mm clear corneal incision. There’s also no need for additional paracenteses. The single-use ring comes in two sizes, 6.25 mm and 7 mm, and is sold in units of six. It’s compatible with the Osher/Malyugin Ring Manipulator 2.0. The ring offers eight points of contact with the iris, making a near-circular pupil.
“The gentle expansion of this ring is ideal for cases where tearing the iris sphincter is a risk,” Dr. Malouf says. He adds that the Malyugin ring is “easy to put in and easy to take out.” His favorite feature of this ring is the smoothness of its material, which he says creates less anterior capsular drag.
“It’s made of 5-0 polypropylene suture, which is firm enough to stabilize the pupil and yet flexible and gentle on the tissue,” explains Dr. Colvard. “Most importantly, it has a low profile. It works like a charm.”
For a video of Dr. Malyugin using the ring, visit aao.org/clinical-video/malyugin-ring-2-0. REVIEW
Dr. Malouf reports no relevant financial interests. Dr. Colvard and Dr. Whitman report no relevant financial interests, but both say they have consulted for Oasis in the past.
1. Al-Hashimi S, Donaldson K, Davidson R, et al. Medical and surgical management of the small pupil during cataract surgery. ASCRS 2018 Review/Update. 2018;1-10.
2. Malyugin B. Cataract surgery in small pupils. Indian J Ophthalmol 2017;65:12:1323-8.


