|
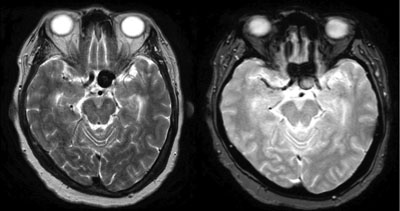
Given the patient’s presentation to the neuro-ophthalmology clinic and prior testing, a broad differential diagnosis for optic neuropathy was considered, although giant cell arteritis and NAION were considered to be most likely. Laboratory testing showed a normal erythrocyte sedimentation rate, C-reactive protein and complete blood count. Magnetic resonance imaging with contrast of the brain and orbits revealed a 1.5 x 1.3 cm left ophthalmic segment internal carotid artery (ICA) aneurysm compressing the pre-chiasmatic left optic nerve along with the optic chiasm (See Figures 1 & 2). The patient was sent directly from the imaging center to the Wills Emergency Room, where the exam remain unchanged from her visit to the Neuro-ophthalmology clinic two weeks prior. An emergent neurosurgery consult was placed for evaluation and treatment, and the patient underwent catheter angiography and endovascular embolization.
Discussion
The differential diagnosis of decreased vision post cataract extraction and PCIOL placement is quite broad. In this particular instance the referring ophthalmologist was concerned for NAION. One early study reported a rate of NAION annually as 10.3 per 100,000.1 A later published retrospective analysis concluded a post-cataract extraction six-week incidence of 34.6 per 100,000 and six-month incidence of 51.8 per 100,000.2 Local vasoactive peptide release and IOP fluctuation during and after surgery could result in inadequate blood supply to the posterior ciliary arteries.3
|

The morbidity and mortality of intracerebral aneurysms lie within the risk of rupture and subsequent hemorrhage and vasospasm. There are 30,000 ruptured aneurysms annually in the United States, with a 40- to 50-percent survival rate.4,6 Of the remaining 50 to 60 percent, approximately 20 percent have no significant neurologic deficits.4,6
Ophthalmologic signs and symptoms of aneurysms include mydriasis, cranial nerve palsies, diplopia, decreased vision and pain. The “gold standard” for imaging an aneurysm is catheter angiography. However, computed tomography angiography and magnetic resonance angiography are more commonly performed due to their overall quality without the risks of traditional catheter angiography.
Size and location have been noted to be two major risk factors for aneurysm rupture. The five-year cumulative risk of rupture in our patient is 14.5 percent, whereas in an aneurysm with a diameter of 7 mm or less, the risk is 0 percent.7 In patients with aneurysms 25 mm or larger, the risk of rupture is up to 40 percent.7 Additionally, aneurysmal dilation of the vertibrobasilar or posterior cerebral circulation and the basilar tip confer an increased risk of rupture.4
Treatment options for intracerebral aneurysms include observation, open microsurgical clip ligation and endovascular coil embolization.6 Observation is generally limited to smaller aneurysms with little risk of rupture or aneurysms located in a difficult point to access. Clipping has been best utilized for a wide-necked aneurysm and confers a 1 to 4 percent mortality rate and an additional morbidity rate of 10 to 15 percent cognitive or physical disability.8 Endovascular coiling, although associated with lower mortality and morbidity rates of 1 to 2 percent and 8 percent, respectively, has resulted in higher recurrence risks.8 REVIEW
The author would like to thank Mark Moster, MD, of the Wills Eye Hospital Neuro-ophthalmology Service, and Joshua Ehrlich, MD, of the Wills Eye Hospital Residency Program for their time and assistance in preparing this case report.
1. Johnson LN, Arnold A. Incidence of nonarteritic and arteritic ischemic optic neuropathy. Population-based study in the state of Missouri and Los Angeles County, California. J Neuroophthalmol 1994;14(1):38-44.
2. McCulley TJ, Lam BL, Feuer WJ. Incidence of nonarteritic anterior ischemic optic neuropathy associated with cataract extraction. Ophthalmology 2001;108:1275-8.
3. Lee H, Kim CY, Seong GJ, Ma KT. A case of decreased visual field after uneventful cataract surgery: Nonarteritic anterior ischemic optic neuropathy. Korean J Ophthalmol 2010 Feb;24(1):57-61. doi: 10.3341/kjo.2010.24.1.57. Epub 2010 Feb 5.
4. International study of unruptured intracranial aneurysms investigators. Unruptured intracranial aneurysms - risk of rupture and risks of surgical intervention. N England J Med 1998;339:1725-1733.
5. Quiros PA, Hedges TR. Vascular Disorders. In Ophthalmology (3rd Edition). Yanoff M and Duker JS (Eds.). Harcourt, London, 2008.
6. Dhar S, Tremmel M, Mocco J, et al. Morphology perameters for intracranial aneurysm rupture risk assessment. Neurosurg 2008;63:185-197.
7. International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial aneurysms: Natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 2003;362(9378):103-10.
8. Johnston C, Higashida RT, Barrow DL, et al. AHA Scientific Statement. Recommendations for the endovascular treatment of intracerebral aneurysms. Stroke 2002;33:2536-2544.


