From the clinical history and exam, the mass appeared to be a rapidly growing lesion with extrascleral extension. The differential diagnosis included metastasis, lymphoma and melanoma. While melanoma can present with extrascleral extension, it generally does not present with such rapid growth. A limited workup for primary lung and prostate malignancy, the most common locations of primary tumors metastasizing to the eye, was negative. Therefore, lymphoma was considered a likely possibility.
|
Laboratory values were remarkable for a low hemoglobin, elevated BUN and creatinine, elevated lactate dehydrogenase (LDH) and elevated total protein. Liver enzymes, thyroid stimulating hormone and coagulation factors were all within normal limits.
Given the clinical and imaging findings, the possible treatment options included: fine needle aspiration biopsy; enucleation; or exenteration. Given the aggressive growth of the tumor and the poor visual prognosis of the eye, the patient underwent enucleation with four orbital biopsies and implantation of a hydroxyapatite implant with allograft.
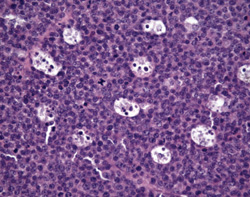
The full globe specimen as well as orbital biopsies were sent for pathology. The orbital biopsies were negative for tumor. The globe displayed angle closure by peripheral anterior synechiae. Microscopically, large atypical lymphocytes and numerous histiocytes were present, with approximately 3.5 mm of optic invasion (See Figure 3). There were tumor nodules underneath the conjunctiva that were not contiguous with intraocular tumor, presumably seeded through the emissary canals. The tumor was highly mitotically active, with 15 to 20 mitotic figures per high-powered field.
Immunohistochemistry findings (immunoglobulin lambda-light chain restriction, IgA heavy chain, CD20 negative, CD79a positive, CD138 positive, MUM1 positive, and PAX5 negative, 95 percent positive Ki67 index) supported the diagnosis of high-grade large cell lymphoma with plasmablastic features. Since it was an isolated tumor, the final diagnosis was plasmablastic lymphoma.
|
Discussion
Plasmablastic lymphoma, according to the most recent World Health Organization classification in 2008, is a diffuse preparation of large neoplastic cells that resemble B immunoblasts, but have the immunophenotype of plasma cells.1 The blastic proliferating B cells have switched on the plasma cell gene expression program.
While cases have been reported in immunocompetent elderly individuals, plasmablastic lymphoma has a high incidence in immunocompromised individuals, particularly those with human immunodeficiency virus and acquired immune deficiency syndrome. In the first reported case series, 15 of the 16 patients were HIV positive, and in the largest literature review of 228 patients, 69 percent were HIV positive.2,3 Median age at presentation is 50 years old.
Plasmablastic lymphoma most commonly presents as an oral mass, but extranodal sites have also been primarily involved as well, including reported cases in the orbit. The pathogenesis is unknown, but it is thought to originate from post-germinal center, terminally differentiated B cells that are in transition from immunoblast state of development to plasma cells. Some have suggested a role for Epstein-Barr virus, as it was present in HIV-associated plasmablastic lymphoma cells in 74 percent of cases in one review.4
Most cases of plasmablastic lymphoma present as advanced disease, in stage III or IV, and most patients die within one year of presentation.3 Without chemotherapy, the median survival is three months. There is no consensus or standard of care for chemotherapy regimens to treat the disease, and it is unclear if treatment with highly active anti-retroviral therapy improves prognosis.5
The patient presented in this review went on to develop multiple subcutaneous nodules. He elected not to have any further workup, and he succumbed to the lymphoma several months after the development of ocular disease. REVIEW
The author would like to thank Carol Shields, MD, and Ralph Eagle Jr. , MD, of the Wills Eye Institute Ocular Oncology Service and Ocular Pathology Department, respectively, for their time and assistance in preparing this case report.
1. Jaffe ES, Pittaluga S. Aggressive B-cell lymphomas: A review of new and old entities in the WHO classification. Hematology Am Soc Hematol Educ Program 2011;2011:506-14.
2. Delecluse HJ, Anagnostopoulos I, Dallenbach F, et al. Plasmablastic lymphomas of the oral cavity: A new entity associated with the human immunodeficiency virus infection. Blood 1997;89:1413–20.
3. Castillo JJ, Winer, ES, Stachurski D, et al. Clinical and pathological differences between human immunodeficiency virus-positive and human immunodeficiency virus-negative patients with plasmablastic lymphoma. Leuk Lymphoma 2010;51:2047-53.
4. Castillo J, Pantanowitz L, Dezube BJ. HIV-associated plasmablastic lymphoma: Lessons learned from 112 published cases. Am J Hematol 2008;83:804-9.
5. Castillo JJ, Winer ES, Stachurski,D, et al. Prognostic factors in chemotherapy-treated patients with HIV-associated plasmablastic lymphoma. Oncologist 2010;15:293-9.


