THE ADVENT OF EPI-LASIK HAS SPARKED A NUMBER OF QUESTIONS in the minds of refractive surgeons: What's the level of postop pain compared to PRK? How fast is the visual recovery? What is the quality of the cut?
In this, the second part in a two-part series on surgeons' clinical impressions of the epithelial separators, physicians share their thoughts on the VisiJet EpiLift and AMO Amadeus II epi-LASIK devices.
VisiJet's EpiLift
This system is produced by Germany's Gebauer company, and is distributed in the United States by VisiJet (Irvine, Calif.).
The EpiLift uses an applanator bar to flatten the epithelium ahead of the device's SureEdge metal separator to help facilitate the creation of the flap-like epithelial sheet that's at the heart of epi-LASIK. The surgeon can vary the size of the flap and hinge, as well as the oscillation rate of the separator from 6,000 to 10,000 rpm. VisiJet recommends 9,000 rpm oscillation. The speed of the head across the epithelium is fixed at 1 mm per second.
This system is produced by Germany's Gebauer company, and is distributed in the United States by VisiJet (Irvine, Calif.).
The EpiLift uses an applanator bar to flatten the epithelium ahead of the device's SureEdge metal separator to help facilitate the creation of the flap-like epithelial sheet that's at the heart of epi-LASIK. The surgeon can vary the size of the flap and hinge, as well as the oscillation rate of the separator from 6,000 to 10,000 rpm. VisiJet recommends 9,000 rpm oscillation. The speed of the head across the epithelium is fixed at 1 mm per second.
 |
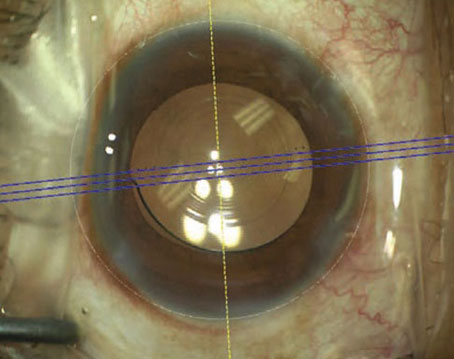
| The EpiLift separator uses an applanator bar to make it easier to separate epithelium. |
Chris Lohmann, MD, of Regensburg, Germany, has performed around 700 epi-LASIK cases with the EpiLift system on patients with up to 8 D of myopia.
"I've had no stromal complications," he says. "I've had two free epithelial flaps. All the other flaps were perfect. We have maybe 15 percent of patients who have grade 0.5 corneal haze at three months, but after three or four months it's gone."
He says re-epithelialization time depends on the patient. "In some patients, we can take the contact lens off on postop day two," Dr. Lohmann says. "In others, though, it takes a bit longer. We can usually take it off around day three."
Interestingly, just as described by other epi-LASIK surgeons, Dr. Lohmann says the vision fluctuates in the immediate postop period.
"On average, on days one and two it's 20/40," he recalls. "On day three it goes down slightly, and then goes up from there. On day seven, everyone has achieved their best vision, I would say."
Dr. Lohmann has also studied a patient cohort to get a sense of postop pain. "If pain is going to be a problem it will be within the first four hours," he says. "And about 20 percent of the patients will tell me that they have some sort of pain that's bothering them. The most important thing is to tell the patients preoperatively that they might experience pain, so that if the pain comes it's not unexpected. But we haven't had long-term pain as can occur with PRK." He says that when the patients rated pain on a visual analog scale from one to 10, no one went over four, and most were between two and four. He gives patients diclofenac tablets postoperatively for pain.
"I've had no stromal complications," he says. "I've had two free epithelial flaps. All the other flaps were perfect. We have maybe 15 percent of patients who have grade 0.5 corneal haze at three months, but after three or four months it's gone."
He says re-epithelialization time depends on the patient. "In some patients, we can take the contact lens off on postop day two," Dr. Lohmann says. "In others, though, it takes a bit longer. We can usually take it off around day three."
Interestingly, just as described by other epi-LASIK surgeons, Dr. Lohmann says the vision fluctuates in the immediate postop period.
"On average, on days one and two it's 20/40," he recalls. "On day three it goes down slightly, and then goes up from there. On day seven, everyone has achieved their best vision, I would say."
Dr. Lohmann has also studied a patient cohort to get a sense of postop pain. "If pain is going to be a problem it will be within the first four hours," he says. "And about 20 percent of the patients will tell me that they have some sort of pain that's bothering them. The most important thing is to tell the patients preoperatively that they might experience pain, so that if the pain comes it's not unexpected. But we haven't had long-term pain as can occur with PRK." He says that when the patients rated pain on a visual analog scale from one to 10, no one went over four, and most were between two and four. He gives patients diclofenac tablets postoperatively for pain.
AMO's Amadeus II
This is the newest addition to the world of epi-LASIK separators, and isn't on the market just yet. The epi-LASIK attachment for the Amadeus II will consist of an epi-LASIK blade holder that attaches to the ordinary Amadeus II handpiece, with a specific epi-LASIK separator that fits in the blade holder for epithelial sheet creation.
Only a handful of surgeons have had access to the Amadeus II separator for a short time as part of a clinical study by AMO. The study has only about a month's worth of follow-up thus far, and not all the data has been analyzed in aggregate form, so the only data available is from clinical impressions and anecdotal cases. A full launch of the product is expected in the fall.
Berlin's Manfred Tetz, MD, has had about six weeks' worth of experience with the Amadeus II epithelial separator in about 20 cases. He has 18 months' worth of epi-LASIK experience in general.
"The quality of the cut with the Amadeus II, as I have used it, has been excellent," he says. "We have been involved in the trials that started around the beginning of the year when [AMO was] still looking for the best configuration of the blade. With the currently available blade, a plastic blade, the cut is very nice." He doesn't report any incidences where the current iteration of the separator has cut stroma.
|
Y. Ralph Chu, MD Related Articles |