 |
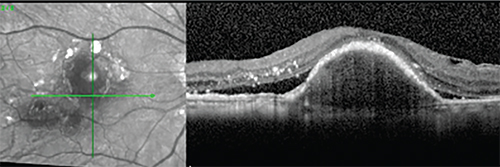
| Figure 1. Incomplete response to anti-VEGF monotherapy. Shown here is a 72-year-old woman with neovascular AMD with persistent subretinal fluid and pigment epithelial detachment following serial ranibizumab and aflibercept injections. |
Pathogenesis of Exudative AMD
To see the potential of combination therapy, it helps to understand the pathogenesis of CNV due to AMD. Unfortunately, the mechanism behind the CNV isn’t completely understood.
The retina receives long-term exposure to light radiation and is therefore vulnerable to oxidative damage. With aging, light-damage accumulation and free-radical injury, the retinal pigment epithelium can be damaged by oxidative products.5 Oxidative stress, in turn, can promote the expression of VEGF mRNA and transcription, supporting theories regarding the important role of oxidative damage in the formation of CNV.6
Apart from the oxidative damage mechanism, many studies have shown that AMD is a chronic, non-specific inflammatory disease.7 Using immunohistochemistry, research has confirmed that AMD eyes have retinal tissue autoantibodies, suggesting that from early to late AMD, retinal antibodies play an important role in the disease’s pathogenesis.8 Additionally, elevated levels of C-reactive protein, a marker of systemic inflammation, have been shown to be a risk factor for AMD.9
Based on our current knowledge of the complex mechanisms of AMD, one can understand that if only anti-VEGF treatment is given, in some cases AMD may not be fully controlled, and clinical observation has confirmed that there is indeed a subset of patients not responsive to anti-VEGF monotherapy.4
The Limits of Monotherapy
PDT with verteporfin was approved in the United States for the treatment of wet AMD in 2000.10 The Treatment of Age-related Macular Degeneration with Photodynamic Therapy (TAP) Study showed that the visual acuity benefit of verteporfin therapy for AMD
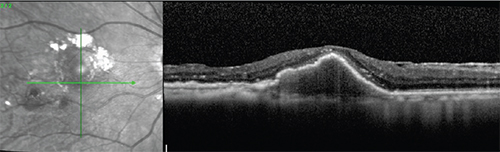 |
| Figure 2. The patient from Fig. 1, showing improvement in exudation after combined anti-VEGF and steroid treatment. There is resolution of subretinal fluid after one dexamethasone intravitreal implant injection in this patient, who had persistent fluid despite monthly anti-VEGF injections. |
Anti-VEGF therapy was an important breakthrough in the treatment of wet AMD and has replaced PDT as the most effective treatment. For example, mean visual acuity changes from baseline were +6.6 and 10.7 letters after 12 months of follow-up in the pivotal MARINA13 and ANCHOR14 trials, respectively. However, 5 to 10 percent of patients with wet AMD didn’t completely respond to anti-VEGF in these studies, even with monthly injections for two years.13,15 This suggests that there is room for improvement in clinical outcomes in at least some patients with wet AMD (See Figure 1). Meanwhile, the possibility of reducing the overall number of treatments is attractive, as long-term injection increases the treatment burden for the patient and could also increase the risk of complications.16 Combination therapy has been suggested by some as a means of addressing these shortcomings.
Combination Approaches
Following is a list of combination therapies currently available to us, and how well they perform.
• PDT and steroid injection. Combination therapy has been used to treat patients with wet AMD for a number of years. The first combination therapy consisted of PDT combined with intravitreal triamcinolone acetonide. A study of this approach demonstrated a reduction in the need for retreatment compared with patients receiving PDT alone.17 Another study showed that combination therapy with PDT and intravitreal TA improved visual acuity and reduced treatment frequency.18 However, this combination therapy was limited by complications such as cataract and glaucoma,19 as well as the relative lack of visual improvement that characterized PDT treatment when compared with anti-VEGF.
• PDT and anti-VEGF. Since anti-VEGF is the most effective monotherapy, some investigators have tried a c
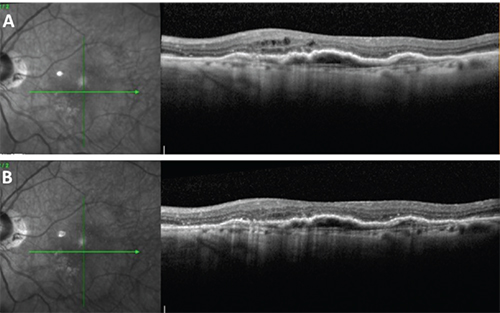 |
| Figure 3. Control of residual exudation with supplemental dexamethasone intravitreal injection in an 85-year-old woman receiving aflibercept injections at baseline. (A) Intraretinal fluid is present despite monthly aflibercept injections. (B) Improvement one month following a dexamethasone intravitreal implant injection. |
• Anti-VEGF and steroids. Both VEGF secretion and inflammation are principal factors contributing to CNV in AMD so, theoretically, combining anti-VEGF with steroid therapy could yield a better outcome than monotherapy. In one study, researchers implanted the dexamethasone intravitreal implant (Ozurdex 0.7 mg; Allergan, Irvine, Calif.) in patients who were already receiving monthly ranibizumab injections who had persistent fluid. The researchers found that the combination treatment promoted complete or partial resolution of fluid in all eyes.4 Another study found that the adjunctive use of the dexamethasone intravitreal implant reduced the need for ranibizumab reinjection during six months of follow-up when compared with sham injection.23 In our practice, too, we’ve combined anti-VEGF with a dexamethasone intravitreal implant for the treatment of refractory wet AMD. In a small cohort of patients, we’ve observed improvement in the clinical course, with resolution of fluid after introduction of steroid to the treatment regimen (See Figures 2 and 3).
In the future, new agents addressing other pathogenic aspects of wet AMD may offer additional benefit in combination with current therapies. In the meantime, combining anti-VEGF and steroid medications may offer a worthwhile treatment option in patients with persistent fluid despite regular anti-VEGF treatment. REVIEW
Xiangbin Kong, MD is a fellow and Jay M. Stewart, MD, a professor in the Department of Ophthalmology at the University of California, San Francisco Medical Center. He may be reached at Jay.Stewart@ucsf.edu.
Dr. Stewart is a consultant for Forsight Vision4. Dr. Kong has no financial interest in any of the products discussed.
1. Studnicka J, Rencova E, Dusova J, et al. [Wet form age-related macular degeneration two years treatment results using anti-VEGF drugs]. Cesk Slov Oftalmol 2013;69:96-101.
2. Kolar P, Vizdova D, Vlkova E. [Photodynamic therapy with visudyne in treatment of wet form of age-related macular degeneration--two years results]. Cas Lek Cesk 2006;145:795.
3. Han DP, McAllister JT, Weinberg DV, Kim JE, Wirostko WJ. Combined intravitreal anti-VEGF and verteporfin photodynamic therapy for juxtafoveal and extrafoveal choroidal neovascularization as an alternative to laser photocoagulation. Eye (Lond) 2010;24:713-6.
4. Calvo P, Ferreras A, Al Adel F, Wang Y, Brent MH. Dexamethasone intravitreal implant as adjunct therapy for patients with wet age-related macular degeneration with incomplete response to ranibizumab. Br J Ophthalmol 2015;99:723-6.
5. Bonne C, Muller A. [Role of oxidative stress in age-related macular degeneration]. J Fr Ophtalmol 2000;23:835-40.
6. Ugurlu N, Asik MD, Yulek F, Neselioglu S, Cagil N. Oxidative stress and anti-oxidative defence in patients with age-related macular degeneration. Curr Eye Res 2013;38:497-502.
7. Parmeggiani F, Romano MR, Costagliola C, et al. Mechanism of inflammation in age-related macular degeneration. Mediators Inflamm 2012;2012:546786.
8. Patel N, Ohbayashi M, Nugent AK, et al. Circulating anti-retinal antibodies as immune markers in age-related macular degeneration. Immunology 2005;115:422-30.
9. Seddon JM, Gensler G, Milton RC, Klein ML, Rifai N. Association between C-reactive protein and age-related macular degeneration. JAMA 2004;291:704-10.
10. Verteporfin therapy of subfoveal choroidal neovascularization in age-related macular degeneration: Two-year results of a randomized clinical trial including lesions with occult with no classic choroidal neovascularization—verteporfin in photodynamic therapy report 2. Am J Ophthalmol 2001;131:541-60.
11. Bressler NM. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: two-year results of 2 randomized clinical trials-tap report 2. Arch Ophthalmol 2001;119:198-207.
12. Blinder KJ, Bradley S, Bressler NM, et al. Effect of lesion size, visual acuity, and lesion composition on visual acuity change with and without verteporfin therapy for choroidal neovascularization secondary to age-related macular degeneration: TAP and VIP report no. 1. Am J Ophthalmol 2003;136:407-18.
13. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med 2006;355:1419-31.
14. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med 2006;355:1432-44.
15. Brown DM, Michels M, Kaiser PK, et al. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: Two-year results of the ANCHOR study. Ophthalmology 2009;116:57-65 e5.
16. Jang L, Gianniou C, Ambresin A, Mantel I. Refractory subretinal fluid in patients with neovascular age-related macular degeneration treated with intravitreal ranibizumab: visual acuity outcome. Graefes Arch Clin Exp Ophthalmol 2015;253:1211-6.
17. Ruiz-Moreno JM, Montero JA, Barile S, Zarbin MA. Photodynamic therapy and high-dose intravitreal triamcinolone to treat exudative age-related macular degeneration: 1-year outcome. Retina 2006;26:602-12.
18. Spaide RF, Sorenson J, Maranan L. PDT with verteporfin combined with intravitreal injection of triamcinolone acetonide for choroidal neovascularization. Ophthalmology 2005;112:301-4.
19. Arias L, Garcia-Arumi J, Ramon JM, Badia M, Rubio M, Pujol O. Photodynamic therapy with intravitreal triamcinolone in predominantly classic choroidal neovascularization: one-year results of a randomized study. Ophthalmology 2006;113:2243.
20. Heier JS, Boyer DS, Ciulla TA, et al. Ranibizumab combined with verteporfin photodynamic therapy in neovascular age-related macular degeneration: year 1 results of the FOCUS Study. Arch Ophthalmol 2006;124:1532-42.
21. Schmidt-Erfurth U, Wolf S. Same-day administration of verteporfin and ranibizumab 0.5 mg in patients with choroidal neovascularisation due to age-related macular degeneration. Br J Ophthalmol 2008;92:1628-35.
22. Dhalla MS, Shah GK, Blinder KJ, Ryan EH, Jr., Mittra RA, Tewari A. Combined photodynamic therapy with verteporfin and intravitreal bevacizumab for choroidal neovascularization in age-related macular degeneration. Retina 2006;26:988-93.
23. Kuppermann BD, Goldstein M, Maturi RK, et al. Dexamethasone intravitreal implant as adjunctive therapy to ranibizumab in neovascular age-related macular degeneration: A multicenter randomized controlled trial. Ophthalmologica 2015;234:40-54.


