In February of this year, refractive surgeons who responded to our National Panel Survey said they'd be more likely to consider an intraocular lens for a high myope than LASIK, and they said so again on this latest refractive surgery questionnaire. Some may also be more willing to give LASEK a chance for such a patient, possibly since it conserves more tissue when compared to LASIK in a high correction.
| Average LASIK Prices and Facility Fees | |||||
| All | Northeast | South | Midwest | West | |
| Price | |||||
| Average | $1825 | $1763 | $1750 | $1820 | $1624 |
| Feb. "03 avg. | $1712 | $1813 | $1830 | $1643 | $1658 |
| Facility Fee | |||||
| Average | $580 | $520 | $647 | $637 | $562 |
| Feb. "03 avg. | $656 | $550 | $950* | $683 | $627 |
| *Only one | surgeon | provided | a facility | fee. | |
These are some of the results of this month's survey of the physicians on our National Panel. This month, 67 surgeons, or 9 percent of the 750 surgeons sampled, responded with their refractive surgery preferences. To see how your opinions compare with theirs, read on.
Myopia Treatment
LASIK is still the most popular procedure for low myopes, with 79 percent of the surgeons responding saying they would use it for a -3 D correction. "It gives a quick result," says a New Jersey surgeon. "And it's safe for this range."
Flushing, N.Y., ophthalmologist R. Scott Russell likes LASIK, but acknowledges that low myopia is the best range for refractive surgery. "At this level, you can get good results with any method—even PRK."
 |
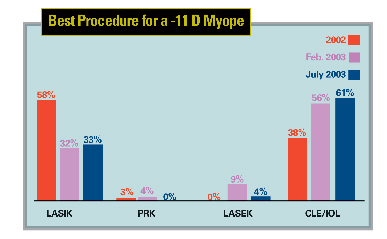
When asked about patients with a high myopic refractive error (in the range of -11 D), though, our panelists have changed their tack compared to 2002. While, last year, most of them (58 percent) chose LASIK for a -11 D case, now only a third say they would do so. Instead, 62 percent say clear-lens extraction/IOL implantation is probably a better idea.
"CLE/IOL doesn't leave a scar in the visual axis," says Fairhope, Ala., refractive surgeon Joseph Gravlee. "And it obviates the need for cataract surgery in the future and the need to suffer from cataract symptoms."
Dr. Russell says he would choose an intraocular procedure because there are "contrast sensitivity problems from corneal remodeling techniques."
"If the eye has enough corneal tissue, LASIK works," asserts Charleston, S.C., physician Sidney Seltzer. "If there's not enough tissue, then a CLE/IOL procedure is better." A surgeon from New Jersey agrees, saying, "-11 D is just too high for a lamellar refractive procedure in most corneas."
A small number of surgeons (4 percent) think LASEK might be worth doing in such a high myope. "We'll see how the results are with LASEK," says a surgeon from Delaware.
Hyperopia Treatment
For a mild hyperope of +3 D, surgeons say they're most comfortable with LASIK. Three-quarters say this would be the best procedure for such a patient.
"The results are still OK with LASIK in these patients," says Dr. Russell. "But, CK may also be an alternative."
"LASIK doesn't give bad results," says Olympia, Wash. surgeon William Waugh.
As the hyperopic refractive error moves higher, into the +5-D range, the trend toward surgeons preferring an intraocular procedure over a corneal one, which began with our February panel, continues. Nearly 70 percent of respondents say they would choose either CLE/IOL or a phakic lens for a +5-D patient, mainly because of the unpredictability of a corneal procedure in this range of hyperopia.
"A lens-extraction procedure spares the cornea," says a Texas ophthalmologist.
 |
Alabama's Dr. Gravlee concurs. "With a phakic IOL, there aren't issues of refractive drift," he says. "A phakic lens also won't interfere with making accurate IOL calculations for cataract surgery later on."
"LASIK isn't dependable at +5 D," says an Ohio surgeon who would choose CLE/IOL.
"At that level, you're pushing the envelope for LASIK," says Dr. Russell, "so I'd prefer either CLE/IOL, or implanting a phakic lens."
Of the surgeons interested in the phakic IOLs currently in the research pipeline, 57 percent are interested in the Staar Implantable Contact Lens, 28 percent in the Ophtec Artisan and 15 percent in the CIBA/Medennium Phakic Refractive Lens.
"I'm not concerned about cataract formation with the Staar ICL," says a physician from Indiana. An Illinois surgeon says he is looking forward to the Staar lens because, "It shouldn't affect the angle or the cornea."
 |
"It's in the best anatomical position," says Dr. Gravlee, commenting on the ICL. "And I feel it's made of the safest material, collamer."
A surgeon from New Jersey prefers the ICL because of "easier insertion."
Dr. Waugh says he's interested in the Artisan lens, however. "It's off of the crystalline lens," he says. "And iris-supported IOLs still look good 25 years later."
Dr. Russell says that he is looking forward to the ThinOptx (Abingdon, Va.) IOL, an experimental lens which may be able to be inserted into an incision smaller than 1.5 mm.
"It's a very innovative new technology," he says. "And, it looks very good for 1-mm incision phacoemulsification."
Presbyopia Treatment
The panelists take a couple of different courses when faced with the perennial challenge of presbyopia.
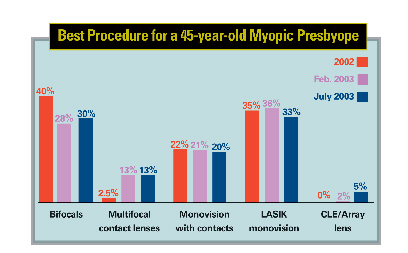
As they did in February's panel report, most of the surgeons prefer either bifocal spectacles (30 percent) or LASIK monovision (33 percent) for a 45-year-old myopic presbyope.
"Bifocals are safe and predictable," says a surgeon from Illinois.
Dr. Russell also prefers to stay away from surgery in these patients, if at all possible. "If they're tolerated, and the patient doesn't have cataracts, multifocal contact lenses or contact-lens monovision, or simple bifocals, may be the best options," he says.
 |
Dr. Gravlee is part of the 20 percent who prefer monovision with contact lenses because he wears contact lenses himself for that purpose. "What is best for me is probably going to be best for my patients, too," he says.
Still, a third of the surgeons like LASIK. "LASIK monovision gives safe, consistent results," says an Indiana surgeon. A New Jersey surgeon agrees, asserting that the procedure offers patients "less of an imbalance between the two eyes and high satisfaction."
One surgeon from California says he will use contact-lens monovision at first, "to check the patient's tolerance," then will move on to monovision with PRK or LASIK if the patient shows he is able to successfully tolerate the monovision effect.
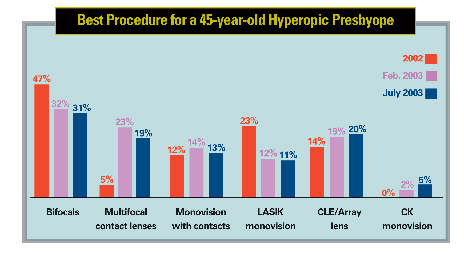
To correct the 45-year-old hyperopic presbyope, 31 percent of the surgeons responding say they would choose bifocals.
"These may give you the best results in this patient," says a surgeon from Michigan.
Nineteen percent of the ophthalmologists say they would use multifocal contact lenses, down slightly from the number in the last survey—23 percent. Dr. Gravlee says he would use them "as a test for multifocal adaptability and to buy time for improved multifocal and accommodative lenses."
Dr. Waugh says he prefers LASIK monovision in such cases because of "patient happiness" with the outcomes of the procedure.
The number of surgeons who would perform a monovision treatment with conductive keratoplasty is up slightly, increasing to 5 percent from 2 percent on the last survey.
A surgeon from New Jersey says this could be a good option because CK is "minimally invasive."