Although stem cells were discovered in the mid-1800s and the subject of experimentation in the early 1900s, it’s only been in recent decades that they’ve truly caught the imagination of medical researchers and the public. Today, our understanding of these cells is expanding dramatically, and research has proliferated as their potential has become clear. Nevertheless, stem cell research is still in its infancy. Because a host of basic questions remain unanswered, research around the world is moving in multiple directions, testing many different possible ways to derive stem cells and apply them in vitro for research and in vivo for treating or preventing disease.
A stem cell is defined as an undifferentiated cell that has the potential to become a number of specific cell types. However, depending on the derivation of the stem cell, its fundamental characteristics may be significantly different. There are four primary stem cell types: embryonic, taken from very early fertilized embryos; parthenogenetic, taken from unfertilized eggs with a simpler genetic sequence for researchers to manage; so-called adult stem cells, found in different organs and designed to differentiate into the cell types found in that organ only; and induced pluripotent stem cells, which are differentiated cells (for example, skin cells) that are coaxed into returning to an undifferentiated state, from which they may then evolve into any number of other cell types. Each type of stem cell has specific advantages and drawbacks that make it better suited—at least in theory—for specific applications.
As is often the case in medical research, the eye has become a popular target. That’s partly because results are typically easier to monitor in the eye than in other organs, and partly because much of the eye in immune-privileged, making it receptive to treatments that might trigger rejection in other parts of the body. Current targets include the retina, cornea, trabecular meshwork and simply stabilizing abnormal blood vessels.
Here, researchers from a dozen different groups around the world discuss their work with stem cells and the eye, explaining their goals, their reasons for choosing the types of cells they’re working with and what they’ve discovered to date.
Embryonic Stem Cells Redux
|

Matthew Vincent, PhD, Advanced Cell Technology’s director of business development, explains that the embryonic stem cell lines they use to make differentiated cells for transplantation are not obtained in the traditional way. “The original technique for obtaining embryonic stem cells involved isolating the inner cell mass from embryos that were left over from in vitro fertilization, embryos that were being thrown away. It was necessary to break apart the embryo, which, as everyone knows, is controversial.
“We don’t obtain our cells in that way,” he continues. “We realized that in vitro fertilization clinics had developed a technique that allows them to take a single cell from a much earlier-stage embryo and use that for genetic testing. This technique, called preimplantation genetic diagnostics, is neither destructive nor harmful to the embryos. In fact, there are 40,000 to 60,000 people in the world who had this single-cell biopsy done to them when they were only eight-cell embryos in a clinic.
“It was Robert Lanza, MD, at our company who figured out that you can take that single cell and generate an embryonic stem cell line from it,” he says. “So in 2005, we generated about a dozen embryonic stem cell lines using this non-destructive technique. By definition, these cell lines can divide indefinitely, so one single cell can now be used to make trillions of doses of retinal cells—or any other tissue in the body. Ultimately, all of our cell therapies will be derived from the embryonic stem cell lines we started back in 2005. If people come to understand this, it should help make them more comfortable with these therapies.”
Dr. Vincent says that to get the stem cells to form the desired type of tissue, they recapitulate the signals that stem cells encounter during the formation of the eye in utero. “Duplicating those in the culture dish causes the stem cells to become RPE cells,” he explains. “The result doesn’t look like an eye; we end up with sheets of lightly pigmented cells. A small, six-wall culture plate, roughly 4 x 6 inches in size, has enough surface area to manufacture 50 doses of cells. So the process can be done on a large scale in a small space. An individual dose is 50,000 to 200,000 cells; it can be cryopreserved so it’s easy to ship; and just as importantly, the injection of the cells into the patient’s eye uses a standard, off-the-shelf cannula, which most eye surgeons are familiar with. The entire procedure, including the vitrectomy, takes 90 to 120 seconds. It’s very straightforward.”
Embryonic Advantage
“We’re currently deriving a number of different tissues from our embryonic stem cell lines that we hope can be used to either reduce the rate of progress of disease or repair and regenerate tissue that’s been damaged by disease such as macular degeneration,” he continues. “Our rationale for treating the RPE is that it serves a host of important functions. It secretes trophic factors that support the photoreceptors; it’s involved in detoxifying the back of the eye; it secretes a basement membrane and is responsible for the health of Bruch’s membrane, the loss of which leads to wet macular degeneration; and it’s pigmented, so it both protects the underlying capillary bed from UV radiation and absorbs light that isn’t absorbed by the photoreceptors, preventing backscatter and thus improving visual acuity. We think that replacing missing RPE cells is the right approach to treating a variety of diseases.”
|
Dr. Vincent admits that embryonic stem cells are not ideally suited for every situation. “Induced pluripotent stem cells make sense when you need patient-specific stem cells,” he says. “We’ve focused on diseases in which allogeneic tissue—tissue from another donor—is appropriate. It’s going into a space in the body that’s generally immune-privileged, where the immune system won’t see it and reject it. But there are a lot of other tissues such as heart or pancreas where that’s not a practical strategy. Because our cells don’t need to be generated from the patient, they represent a more commercially tractable model, but iPS cells will still play a big role in stem cell therapies.
“In the meantime, however, there are still issues with iPS technology that need to be resolved,” he says. “For example, embryonic stem cells can divide indefinitely, but iPS lines will typically stop dividing after two to 20 passages. You also see a high level of mutation occurring in a lot of iPS lines, and some lines have displayed a problem called epigenetic memory, where some of the cells spontaneously differentiate back to the type of tissue you made them from. The science is intriguing, but I think the reality is that we still have a ways to go before that approach is perfected.”
He notes that it’s a huge advantage that the RPE layer is immune-privileged. “That means you don’t have to match the donor cells with the patient’s, so you can create a therapy that you can manufacture in one place, store and then ship to the clinics where it will be injected,” he says. “You don’t have to go through the process of trying to match up donors or harvest tissue from the patient to make new RPE cells.
|
Early Results
Dr. Vincent says early results of the current trials have already been published. “We have a dry macular degeneration trial and a Stargardt’s macular dystrophy trial in the United States, and a Stargardt’s trial in Europe,” he notes. “The results so far have confirmed the treatment’s safety; we’ve seen no evidence of inflammation or formation of the wrong types of tissue. We’ve now treated a total of nine patients with the same result—no adverse effects whatsoever.
“Even though these are Phase I studies, we’d hoped that we could find some evidence that the cells were surviving, engrafting at the right anatomical location and persisting,” he says. “In each case we’re dealing with late-stage patients, so we didn’t expect to see any impact on their visual acuity. Now, with more than a year of data on our first two patients, we’ve seen evidence of engrafting and persistence—and we’ve also seen both subjective and objective evidence of improved visual acuity across the board, for all patients. Subjectively, patients are telling us that they have better contrast sensitivity. In some cases colors that had faded, particularly in Stargardt’s patients, have started to come back. And in many cases we’ve seen measurable changes in visual acuity.”
Dr. Vincent says the first Stargardt’s patient went from hand motion only to being able to read three lines on an eye chart. “That improvement has persisted for 12 months,” he adds. “So we’re seeing functional evidence that the cells are doing what they’re supposed to do, and it’s persisting for a long time. If this therapy works the way we hope it does, it’s conceivable that patients might only have to go back and get a cell injection once every couple of years. Some patients might be able to go a lifetime with a single injection.
“Our end goal is to get this product to the point at which it can be used in patients who are just beginning to have signs of these diseases,” he says. “We’d like to resurface, and as a consequence recapitulate, the structure of the RPE layer before there’s been any substantial loss of photoreceptors.”
Dr. Vincent adds that the company is also making a number of other cells for use in the eye. “We have a brand new type of photoreceptor progenitor cell that we’re excited about,” he says. “This one has characteristics that have not previously been described in the literature. It can form either rods or cones, and because it’s fully differentiated when we inject it, it’s extremely unlikely to turn into a different type of tissue. We think that from a safety perspective, this is the appropriate candidate cell to use in late-stage macular degenerative disorders, where you want to be able to replace photoreceptors that were lost.
“We’ve also been working on a number of protein therapeutics that have potentially neuroprotective and maybe even regenerative capabilities with regard to photoreceptors and other layers of the eye,” he adds. “These are not cell therapies, but biologics. They reduce the impact of stress on the photoreceptors, and may possibly trigger regeneration. And, we have a corneal endothelium program. We can now make corneal endothelial cells capable of secreting Descemet’s membrane and forming sheets of cells in the culture dish. This is currently in animal studies, and we’ve seen a lot of encouraging results to date.”
|

Growing a Retina
Embryonic stems cell in vivo end up as all kind of different organs, and it turns out that it’s possible to coax them to develop into organs—at least partly—in vitro. A number of groups are experimenting with that potential.
| ||||
Dr. Gamm says his group is particularly interested in two applications. “One is using iPS cells to model diseases,” he explains. “We take individuals who have certain inherited retinal degenerative diseases, generate iPS cells from them, forward-engineer those to retinal cells and then study the retinal cells in a dish. It’s as close as we can come to getting a biopsy from the patients while they’re still alive. This should help us pinpoint areas in which we can intervene to slow down or perhaps reverse the disease process.
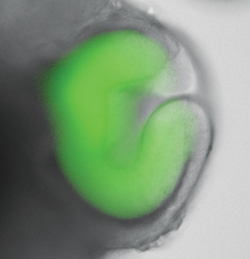
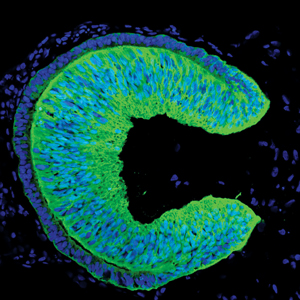
“The other application we’re interested in is the possibility of cell replacement—generating cell types that might be used to improve retinal and visual function in patients with retinal damage or disease,” he says. “Our laboratory published an article last year showing that using either embryonic stem cells or iPS cells, we can grow and isolate very early retinal structures, akin to optic vesicles. These are hollow structures, similar to what you see when the optic vesicle evaginates from the neural tube early in development. Furthermore, these structures go on to produce cell types found in the neural retina, including photoreceptor-like cells.
“More recently we’ve shown that a certain percentage of these structures actually self-assemble to some degree, and form crude layers—in a dish,” he continues. “They form relationships to one another that are similar to what one would see in a developing human retina.” Dr. Gamm notes that this work has been verified, using human embryonic stem cells, by Yoshiki Sasai, MD, in Japan.
“So far, no one has hooked the structures up to a damaged or diseased retina, or shown that they can restore vision,” notes Dr. Gamm. “But that’s one of the next big steps. Of course, many hurdles remain. For example, what happens at the interface when you put these cells in a host retinal environment? Retinal disease is very rarely a matter of just one missing part, with everything else patiently waiting for the new part to be plugged in. And certain diseases will be much more difficult to address with stem cell replacement. So having a better understanding of the environment into which you’re going to place that new cell is imperative. I’m very hopeful that there will be tangible clinical benefits from this technology in the near future; but it’s not going to be a home run right off the bat.
“Furthermore, there are immune issues that need to be dealt with,” he adds. “Do iPS cells taken from the individual being treated give you an immunologic advantage? We assume so, but that needs to be addressed. What about the survival of the cells? Are we actually replacing dysfunctional cells, or are we generically supplying neurotrophic factors beneficial to the remaining cells? Is there a sweet spot in terms of timing that’s more conducive to cell replacement? Is there a potential to form tumors, and if so, how do you get around that? Safety has to be the highest priority.”
Growing an Optic Cup
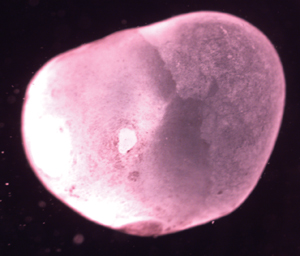
Along these same lines, Yoshiki Sasai, MD, PhD, and colleagues at the RIKEN Center for Developmental Biology in Kobe, Japan, have been able to generate miniature versions of several organs, including a human optic disc, using embryonic stem cells. “We recently succeeded in making a few types of three-dimensional organ buds from embryonic stem cells in culture, including an optic cup, pituitary gland and cerebral cortex,” he says. “Importantly, these complex tissue architectures form in vitro by self-organization. Embryonic stem cell aggregates spontaneously grow into these shapes under the control of their internal program, which was really surprising to us.” The miniature optic cup included a layer containing a significant number of light-responsive photoreceptor cells.
To get the cells to develop into the desired organ type, Dr. Sasai says they use different culture media optimized to trigger specific differentiation. “We try to control ‘positional information’ within the developing central nervous system,” he explains. “The positional information is controlled in vivo by a combination of multiple secreted factors such as bone morphogenetic protein, wingless protein, fibroblast growth factor and sonic hedgehog homolog—so-called growth factor proteins. We empirically optimize this combination for each cell type. In addition, in the case of an optic cup, since its development is highly dependent on basement membrane signals, we added a basement membrane protein called laminin to this culture.”
|
Dr. Sasai notes that there are limits to growing organs using this method. “Since this is an in vitro system in which the organ does not receive blood circulation, organ buds can be grown up to a few millimeters—several millimeters at most,” he says. “However, even in vivo, embryonic organ buds are generally less than 1 mm when they’re first formed. Therefore, a practical strategy would be to produce mini-organs in vitro by self-organization and then grow them in vivo by transplantation.”
Dr. Sasai notes that his group is currently focusing on the mechanisms of organ self-organization. “This is truly full of wonder,” he says. “There are complex dynamic networks operating, and we are trying to understand them via multiple approaches. And, we’re currently implanting hESC-derived 3-D retina tissue into rodent and primate eyes. Primary targets are retinal degenerative diseases such as retinitis pigmentosa, in which the neural retina is slowly degenerating.
“This is a very promising approach,” he concludes. “We believe that self-organization methods will be a major core technology in next-generation regenerative medicine, enabling the use of highly functional and self-sustainable complex tissues for transplantation. In addition, studying the process of self-organization will tell us about the still unknown world of cell sociology, where much higher levels of ordered phenomena occur on their own than we’ve ever seen before.”
Generating Corneal Tissue
Researchers at International Stem Cell Corporation (ISCO) in Carlsbad, Calif., collaborating with researchers in India, are working on using stem cells to generate corneal tissue. Rather than embryonic stem cells or iPS cells, ISCO uses human parthenogenetic stem cells, which are derived from an unfertilized human egg, an approach the company believes has certain advantages over the other alternatives.
“We’ve approached the development of stem-cell-derived corneas from two different directions,” says Ruslan Semechkin, PhD, vice president of research and development. “First, we’re deriving and characterizing corneal tissue, including layers of different cell types, from stem cells; and second, we’re directly deriving corneal endothelial cells using a new differentiation method we’ve developed.”
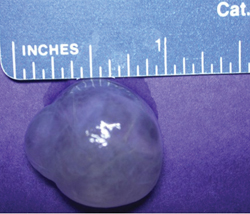
Jeffrey Janus, senior vice president of ISCO, notes that the first approach uses spontaneous differentiation techniques and results in a multi-layered tissue orb containing multiple cell types. The orb strongly resembles a cornea. (See examples, left.) “These orbs have an epithelial layer and a stromal layer separated by what looks like a Bowman’s layer,” he says. “The first application of these orbs is likely to be in toxicology testing, but ultimately we may be able to develop a therapeutic product, possibly for use as a graft. The second program, headed by Dr. Semechkin, uses a directed differentiation methodology to create corneal endothelial-like cells from stem cells, using protocols developed by ISCO that can specify how stem cells behave.”
“Ultimately, we hope to generate a complete cornea,” says Dr. Semechkin. He notes that parthenogenetic stem cells have several advantages over embryonic stem cells, including immune-matching. “PSCs created from individuals who carry a common immune type, or haplotype, can be made to match millions of people,” he says. “Admittedly, this may not be too important for the cornea, because of its immune-privileged position at the front of the eye, but it may be important for other therapeutic applications. The second major advantage is the source of derivation. To obtain an embryonic stem cell, you traditionally have had to destroy an embryo. ISCO derives stem cells from unfertilized eggs, eliminating this ethical issue.
“Another advantage of PSCs is that they remove any concern about the patient’s own cells containing the same genetic disorders that may have contributed to the problem in the first place,” he continues. “With PSCs, we can immune-match the derived cell, and ensure, via genetic screening, that the new cells do not carry the genetic disorder responsible for the original problem. The bottom line is that we believe PSCs can do anything embryonic or iPS stem cells can do. I think, in time, PSCs will be the main type of stem cells used.”
Mr. Janus admits that the corneal tissue they are currently producing has a shelf life. “We can produce up to 30 orbs per batch, but they are short-lived,” he notes. “Although they grow as large as 10 to 15 mm in diameter, they slowly decline if they’re not used. So when they reach a certain size we send them for study or fix them. And we still have some challenges we’re trying to solve, including the thickness of the stromal layer, which is very fragile right now. Also, we have evidence suggesting that the orbs contain Descemet’s membrane and an endothelial layer, but we haven’t definitively proved that yet.”
“That’s one reason we’ve taken this dual approach and are deriving endothelial cells separately,” adds Dr. Semechkin. “We can use the cells separately for treatment and therapeutic purposes, but they can also be used with our corneal orbs, as a third layer.”
Dr. Semechkin notes another recent development. “We now believe we may have found limbal stem cells in the orbs,” he says. (Unlike pluripotent stem cells, these will only develop into eye tissues.) “This is exciting, because if we can isolate and purify these cells, they could be especially helpful for individuals with damaged corneas. However, we still have the challenge of scaling up production to sufficient numbers, and we still have to prove that they truly are limbal stem cells.”
Mr. Janus adds that they are also working on producing retinal tissue from PSCs. “As Dr. Semechkin mentioned, the front of the eye is immune-privileged, largely because of the lack of vascularization, but there is a greater chance of immune rejection issues with cells in the back of the eye where the tissue is more vascularized,” he says. “Because PSCs can be immune-matched, they may have an advantage over using embryonic stem cells that are not immune-matched. However, if immune rejection is going to be a problem, it’s likely that it will be a long-term issue. For now, I think the jury is out.”
A Carpet of Cells
One of the major stem cell research projects currently under way is the London Project, headed by Peter Coffey, PhD. Its focus is on finding a treatment for macular degeneration—particularly the dry form. “Back in 2007 we started a five-year plan to take a human embryonic stem cell therapy to the clinic,” explains Dr. Coffey. “Our goal was to produce a patch of RPE that we could put in the back of the eye in patients who had macular degeneration. In 2009, we also set up a partnership with Pfizer Regenerative Medicine to help us accomplish this. We’re currently in the process of finishing all the preclinical and toxicology studies needed for regulatory approval here in the U.K.”
Professor Coffey says the cells they’re using are from a human embryonic stem cell line produced at Sheffield University, taken from donated, fertilized blastocysts resulting from in vitro fertilization. “Our preclinical study data, using an animal model, were as expected,” he notes. “We’ve had no issues relating to tumorgenicity. The safety and toxicology data have been very positive.
“We produce RPE cells from the embryonic stem cells,” he explains. “Rather than just delivering a suspension of these cells into the eye, we deliver a carpet of RPE cells, about 3 by 6 mm. That’s large enough to cover the entire macula. We deliver the carpet in a single layer—fully differentiated and oriented in the right direction, pointing towards the photoreceptors. We consider this the best way to deliver the RPE cells, so they’ll function like the cells that have died because of the disease. The carpet of cells is surgically delivered using a tool we’ve developed. The membrane is rolled into a tube, and it has memory, so when it’s pushed out it unfolds flat. We place it into the subretinal space. The procedure is very similar to an operation done for retinal detachment.”
Professor Coffey says this work was inspired by early work using a patient’s own retinal cells. “We’ve lasered patches of RPE from the peripheral retina and placed them into the central area,” he says. “We have examples of long-term visual recovery for up to eight years in those patients. That’s what gave us confidence that if we can produce these patches in other ways, by using stem-cell-derived RPE, then we’d expect as good, if not better, results.”
Stabilizing Retinal Vessels
Martin Friedlander, MD, PhD, professor in the department of cell biology at the Scripps Research Institute in La Jolla, Calif., and chief of retina services in the division of ophthalmology at Scripps Clinic, explains that their stem cell research involves using several types of stem cells for different purposes, including using iPS cells to treat atrophic macular degeneration and using stem cells derived from bone marrow, cord blood or peripheral blood to stabilize abnormal vasculature, and for neurotrophic rescue in retinal degeneration and neovascular eye diseases.
|
“As the blood vessels become diseased, they can no longer support the neurons in the style to which they have become accustomed,” he continues. “So in both neovascular macular degeneration and diabetic retinopathy, our thinking shifted several years ago from bashing the abnormal blood vessels to perhaps nurturing and stabilizing them using stem cells.”
Dr. Friedlander says this led them to identify populations of stem cells that exist in normal adult bone marrow and peripheral cord blood, known as endothelial or myeloid progenitor cells. “When placed in the appropriate environment, these cells can stabilize and prevent deterioration in abnormal blood vessels,” he explains. “We found that whenever we put these populations of stem cells into eyes with damaged blood vessels, we observed both vascular and neurotrophic rescue. Photoreceptors which would have deteriorated were stabilized as well.”
iPS and the RPE
“The other project we’re engaged in involves taking normal adult skin or somatic cells and generating induced pluripotent stem cells,” says Dr. Friedlander. “This has traditionally involved introducing four transcription factors into the cells using retroviral vectors to get them to regress back to a pluripotent stem cell state. Once the cells are in that state, you can then, in theory, differentiate a variety of replacement parts for different parts of the body.
“The problem with this approach is that you have to use retroviruses, which can cause problems themselves,” he continues. “In addition, of those four transcription factors, two are potential oncogenes. So our approach has been a little bit different. We’ve looked at the use of episomal vectors; that is, ones that don’t integrate into the genome. And we’ve also looked at replacing those transcription factors with small molecules, or chemicals. We recently demonstrated that we can replace three of the four transcription factors with small molecules and get very nice iPS cells which we can then differentiate into RPE. Putting that tissue into rat models of RPE degeneration produced very nice anatomic and functional rescue.”
Dr. Friedlander notes that other groups are trying similar grafting approaches, but most are using embryonic stem cells. “While that has advantages, the downside is that the eye is not totally immune-privileged,” he points out. “In current clinical trials, those cells are being injected into patients who are immunosuppressed. So it’s probably not something you want to do chronically in a healthy patient.”
Dr. Friedlander says they still have to determine whether they can generate healthy RPE cells from adults who have macular degeneration. “Theoretically, these patients will be in their 40s and have high risk factors or early signs of atrophic macular degeneration,” he says. “The work we’ve already published was done with fetal or neonatal fibroblasts which were made into iPS and then RPE. The question is, does an adult cell have that same potential? So far we’ve been able to make the iPS from adult stem cells; in a few weeks we’ll know whether they can turn into RPE cells. If we can overcome that hurdle, then I think we’re on the path to the clinics.”
|
“We generate virus-free stem cells from skin fibroblasts of the macular degeneration patient using a small skin biopsy,” she continues. “We then differentiate the stem cells into functional RPE using specific molecules and media. We’re currently investigating to see whether the origin of the cells affects the efficiency and functionality of the stem-cell-derived RPE. For example, we want to see whether skin fibroblasts or corneal fibroblasts will have equal potential to make bona fide RPE.
“We hope to achieve our goals within two to five years,” she adds. “This field is very competitive and many other investigators are also working on using stem cells to address macular degeneration. However, the reality is that AMD is multifactorial and a complex disease, so it will probably take significant effort from several groups of investigators to answer fundamental questions related to the etiology of AMD and to find a cure for this devastating disease.”
Regarding whether adult stem cell offshoots can last as long as embryonic stem cell offshoots, Dr. Friedlander says that’s not clear. “All I can tell you is that in the rat models we’ve looked at, the rescue effect appears good out to eight months so far, which is equivalent to a couple of decades in a human. If you put these in a patient in his 60s and he gets 20 or 40 years out of those cells, that’s pretty significant.” He adds that iPS cells reverting to their previous cell type is not something he has observed. “We’re not selecting stem cells; we’re selecting already differentiated RPE cells. If your population is 99.9999 percent pure RPE, could they revert back? It may be possible, but we haven’t observed that.”
Dr. Friedlander says the team at Scripps hopes to be ready for Phase I clinical trials of both procedures within the next two to three years.
Bone Marrow and the Eye
Another source of stem cells is bone marrow. This approach is favored at NeoStem, Inc., located in New York City, where researchers are working with Harvard’s Schepens Eye Research Institute. “All stem cells are not alike,” explains CEO Robin Smith, MD. “These cells, which we call very small embryo-like stem cells, or VSELs, are very early, immature cells that are preserved in the bone marrow. They appear to have the ability to become many different cell types, and because they are the patient’s own cells, the body doesn’t reject them. We use bone-marrow derived stem cells for our cardiac therapy that’s in development. In that situation, we take stem cells from a person’s bone marrow a few days after a heart attack and inject them into the infarct-related artery, to help prevent worsening of heart muscle function resulting from the damage in the heart.
|
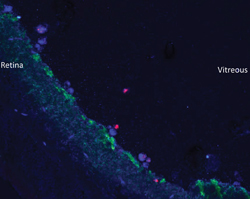
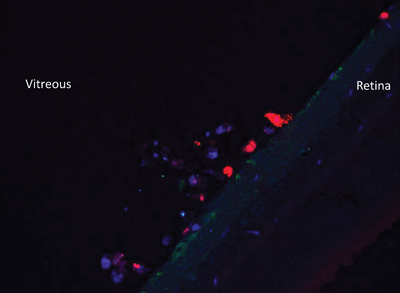
“Our preclinical work indicates that these cells can also become the cells that are found in the eye, leading us to believe that this could have an impact on a number of eye diseases,” she continues. “We’ve been able to isolate these purified cells and inject them into the vitreous humor. They move to the areas where they’re needed, become engrafted to the tissue and turn into the cells that are needed locally to fix whatever is damaged. Because they’re so potent, it appears that you don’t need a lot of them.”
Dr. Smith notes that they are not attempting to induce changes in the cell, as is done with iPS cells. “We’re using cells that already exist in the body,” she points out. “We isolate and purify those that will work for the indication, but we don’t manipulate them. We just put them into the area where they can become engrafted and differentiate into the cell types you need to repair the damaged tissue. Because these are your own cells, they’re safe. Once we demonstrate that, we hope to move on the clinical trials quickly.”
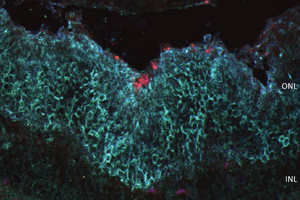
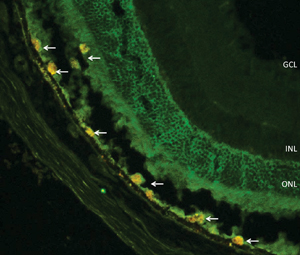
Dr. Smith says that their eye research has focused on repairing damage in the RPE. “Our preclinical animal model research, done with the Schepens Institute, has shown that the cells survive and persist [after injection]; they integrate into the RPE and other layers of the retina and have markers present that suggest that they’re differentiating into the cell types that are needed,” she says. “We’ll be doing more studies to confirm these findings.
“Stem cells have been used for 30 years in bone marrow transplantation,” she adds. “We’re just taking that work further, seeing how these cells can be used to repair damaged tissues in areas such as the eye, heart muscle and other tissues.”
Stem Cells from the RPE?
Researchers at the Neural Stem Cell Institute, located in Rensselaer, N.Y., have discovered a way to isolate stem cells from an individual’s RPE. Sally Temple, PhD, co-founder and scientific director of the institute, notes that under normal circumstances, cells of this type are largely dormant and persist throughout life. “People have extracted RPE from human eyes and cultured it for many years—we certainly aren’t the first,” she says. “Our insight was that it’s a subpopulation of the RPE that’s capable of producing these beautiful cultures—about 1 percent of the cells in an RPE extract. Isolating and studying these cells should provide some answers about how to activate them for benefit and how to control them if they go awry in certain disease states. We’re currently doing some deep sequencing to get a thorough understanding of the composition of these cells.”
|
Dr. Temple says one of the biggest surprises they’ve encountered is that the same cells that produce RPE can also produce mesenchymal progeny such as you would find in bone marrow. “These RPE cells are capable of generating three different mesenchymal progeny—cartilage, fat and bone-forming cells,” she explains. “This is interesting because there are several ocular diseases in which you see mesenchymal-type cells in the eye, such as proliferative retinopathy or macular pucker. Now that we know that RPE cells can produce those cells, we may be able to determine how those progeny form in the eye and find ways to deter their formation.”
Dr. Temple says they are now close to generating cell lines based on the cells they’ve isolated. “We can generate about 108 cells from an individual donor, which should, in the future, allow us to treat many patients from each line,” she notes. “In the eye you need relatively few cells to have a functional impact.
“A number of companies are working hard to pioneer the use of stem cells for treating diseases such as macular degeneration; we see our cells as an alternative approach,” she continues. “The RPE stem cells have a more limited plasticity than a human embryonic stem cell—they’re geared to make RPE. Of course, we don’t know yet whether that will make these cells better or worse at addressing retinal disease than embryonic cells. In any case, being able to potentially draw healthy RPE stem cells from the periphery of an eye, enrich them and place them back in the diseased area of the retina could have the huge advantage of eliminating the potential need for immunosuppressive therapies.”
Dr. Temple adds that they are also working to use these cells to generate dry macular degeneration disease models. “Instead of pushing the cells into becoming healthy RPE, we’re taking some of the cells and changing them into macular degeneration-like tissue in a dish,” she explains. “We hope this will be valuable for drug screening. Animal models aren’t always perfect, so it would be nice to supplement the animal models with human cells in the culture dish.”
Another Source: The Brain
StemCells Inc., located in Newark, Calif., has pioneered the discovery and development of a proprietary, purified and expandable population of human neural stem cells that are extracted from donated fetal brain tissue. “We’ve shown in animal models that these cells can do amazing things, such as restoring lost function in animals who’ve had a spinal cord injury,” says Martin McGlynn, president and CEO of the company. “We’ve found that these cells can remyelinate axons that lack myelin; preserve visual acuity in animals that would otherwise go blind; and enhance memory and improve synaptic density in the hippocampus in Alzheimer’s-disease-relevant models. It’s a remarkably powerful technology.”
Mr. McGlynn explains that the scientific founders of the company postulated that stem cells might be found in specific organs, as opposed to just bone marrow, and established the company to investigate that hypothesis, with a focus on the brain, liver and pancreas. “The developing brain is known to be neurogenic, so the initial research was done using cells derived from donated human fetal brain tissue, because of their innate ability to expand and differentiate into all three cell types of the central nervous system,” he says. “Now we’ve proven that these cells give rise to all of the cells of the central nervous system. What’s fascinating about them is that you can put them into a mouse brain and they’ll be submissive to the mouse host and respond to the microenvironment, and yet maintain their human phenotype. ”
Mr. McGlynn notes that although some groups are trying to address macular degeneration by replacing dysfunctional RPE cells with transplanted stem-cell-derived RPE cells, his company’s approach is very different. “Our approach is to protect the photoreceptors before they degenerate and die,” he explains. “By transplanting the cells into the subretinal space we support the RPE layer and help preserve it. Our cells may also be expressing soluble factors that enable the process of neuroprotection. Furthermore, there’s reason to believe that these cells will have an enduring effect, so this could be a one-time intervention.”
Mr. McGlynn says that they can generate hundreds to thousands of patient doses from one single donated tissue, depending on the particular application. “The cells remain as undifferentiated human neural stem cells while cryopreserved in our cell banks,” he explains. “When we’re ready to send cells to the patient, we simply extract the number of doses we need. We have sufficient cells in the bank to go all the way to commercialization for macular degeneration.”
With this type of allogeneic approach, however, there are some immune system considerations. “To ensure that the cells are not rejected by the host, we administer a very light and temporary regimen of immunosuppression,” explains Mr. McGlynn. “This is nothing like the immune suppression regimen used during a liver or kidney transplant. And when the immune suppression is stopped, the cells seem to continue to do fine, as evidenced by brain autopsy data obtained from a Batten’s patient enrolled in an earlier trial who succumbed to the natural progression of that fatal disease two and a half years post-transplant.
“The FDA has recently approved our clinical trial, designed to evaluate the safety of the cells transplanted into the eye and determine their effect on visual acuity in patients with geographic age-related macular degeneration,” he adds. “We’ve initiated the study and expect to implant our first patients soon. We’ll be placing the cells into the sub-retinal space in the most affected eye, with the other eye as a control. We expect it will take up to two years to complete the study and report the data, with interim evaluation of safety and clinical effect along the way.”
Systemically Applied
Stemedica, based in San Diego, is a licensed manufacturer of allogeneic adult stem cells. “We currently produce two types of allogeneic adult cells,” says David M. McGuigan, vice president of marketing and business development.
“The type we manufacture in the United States is a bone marrow-derived ischemia-tolerant mesenchymal stem cell, from young donors aged 19 to 24. It’s processed in a hypoxic, low-oxygen environment from start to finish, which seems to produce the most beneficial treatment results. Most of our research, and research being done by those using our cell in clinical trials around the world, uses this type of cell. We also produce an ischemia-tolerant neural stem cell in our lab in Switzerland, and we hope to have an RPE cell available in the marketplace next year.”
|
Alexei Lukashev, PhD, director of the laser stem cell division and head of ophthalmic activities at the company, says the company is developing and manufacturing stem cells for a number of basic applications, including cardiology, neurology and ophthalmology. “In the eye we’ve decided to focus on posterior eye applications, especially the retina,” he says. “In the long run we hope to develop treatments for retinitis pigmentosa and macular degeneration. In the short run, we hope to help address diabetic retinopathy and neuropathy. Our work is based upon the results of preclinical studies that we conducted, primarily in Moscow, where we work with the Fyodorov Eye Institute.”
Dr. Lukashev says early results using intravenous injections, rather than injections into the eye, have shown promise addressing these diseases. “We injected six patients who had diabetic retinopathy or diabetic neuropathy and followed them for three years,” he explains. “Although we didn’t detect a change in visual acuity, there was improved blood flow in the periphery of the retina, and the safety of the treatment was confirmed. We submitted this data along with our protocols to the FDA, and we’ve been approved for a Phase I/II clinical trial using IV injection of mesenchymal stem cells in the United States.”
Another interesting part of Stemedica’s early work involved using a laser to draw stem cells in the eye to desired locations. “The idea was to cause mild, transient damage to the retina,” Dr. Lukashev explains. “The damage generates a signal that attracts the cells. We’re continuing to pursue this approach, but in order to get approval for a study we have to first prove that the stem cells are effective and then show what effect the laser has on the retina.”
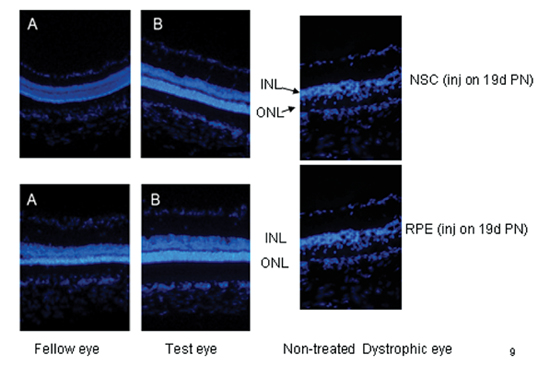
An additional finding that has been confirmed by several animal studies, according to Dr. Lukashev, is that injecting cells into one eye appears to produce beneficial effects in the fellow eye. (See chart, above.) “We consider this a very important finding,” he says. “It could possibly provide a way of treating a patient. For example, if a patient has lost most vision in one eye, the other eye could potentially be treated with maximum safety by injecting the cells into the worse eye, treating the better eye indirectly. We don’t yet fully understand how it happens, but we’re currently working with the animal model to figure that out.” REVIEW


